
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Vergara Ramos J, Ramírez Raposo R, Viejo Almanzor A, Pérez Monzú A, Rodríguez Ramos C. Alternative use of the Salem probe, thinking outside the box. RAPD 2026;49(2):65-67. DOI: 10.37352/2026492.5
Introduction
Colonic decompression is a therapeutic strategy indicated in various conditions that cause acute colonic dilation, such as Ogilvie’s syndrome, colonic volvulus, and malignant obstruction. The goal of endoscopic decompression is simply to reduce the diameter of the colon and thereby the tension on its wall, thus allowing blood flow and enabling the neural and muscular systems to resume peristaltic movement[1]. This can be performed via simple colonoscopy or with the subsequent placement of a transanal decompression tube, with the latter having higher rates of clinical success[1],[2].
Typically, this decompression is performed via suction during colonoscopy and by placing a multi-perforated tube with the aid of a guide catheter and wire guide marketed for this purpose; however, these are not always available in all hospitals.
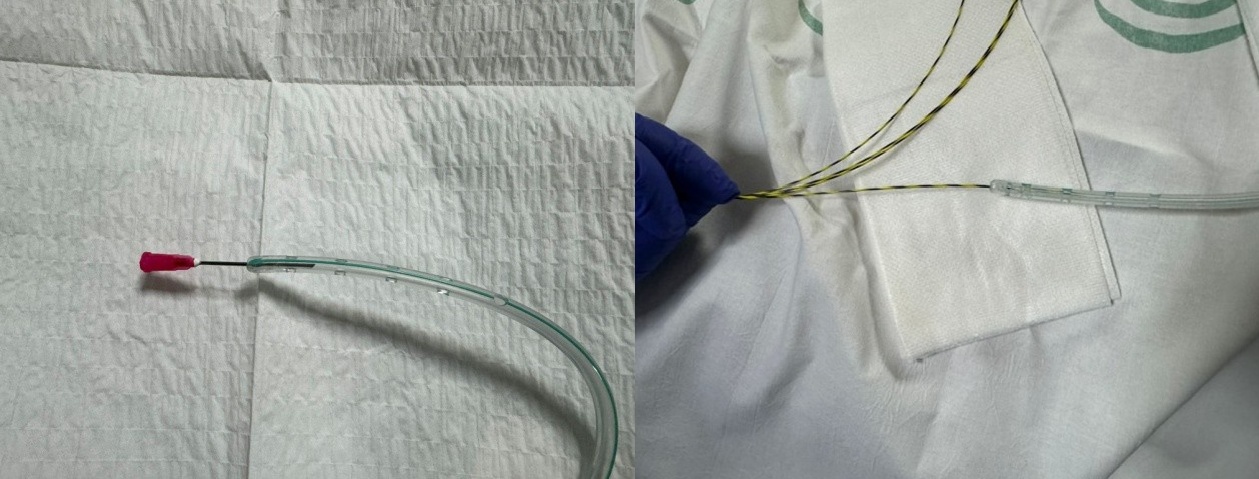
We present an alternative using a Salem tube perforated at its distal end, placed over a guide (Figure 1) in two different clinical scenarios.
Clinical case 1
A 62-year-old man with extensive ulcerative colitis being treated with azathioprine, mesalazine, and golimumab was admitted for intestinal subocclusion. An abdominal computed tomography (CT) scan was performed, revealing a complete stricture at the rectosigmoid junction of unknown etiology (inflammatory versus neoplastic).
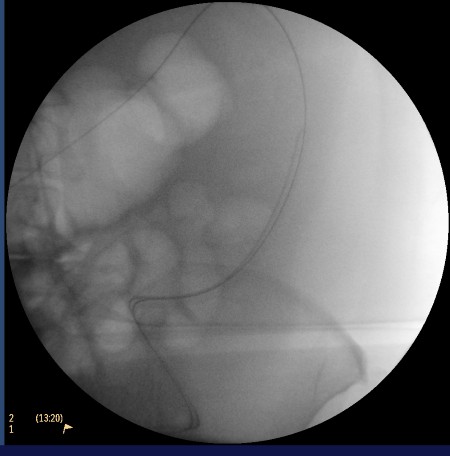
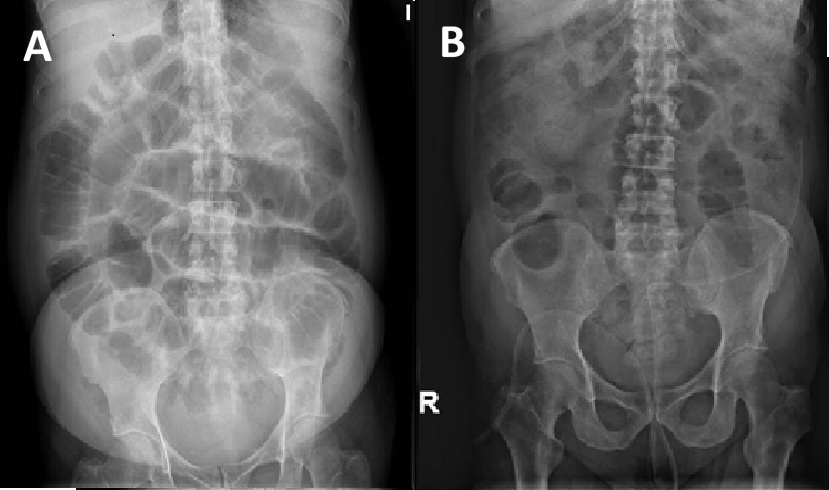
A colonoscopy was performed, revealing stenosis 30 cm from the anal margin with ulcerated and friable mucosa, without a clear neoplastic appearance. Biopsies were taken, and colonic decompression was performed by passing a guidewire through the stenosis under radiological guidance. We injected contrast via the catheter to confirm the luminogram, and after removing the endoscope, we placed a 16-French Salem-type multi-perforated tube over the guidewire (Figure 2), achieving gas release and decompression of the colon(Figure 3). The tube was maintained with saline irrigation on a rotating schedule until histological confirmation of a neoplastic origin, after which a colostomy was finally performed.
Clinical case 2
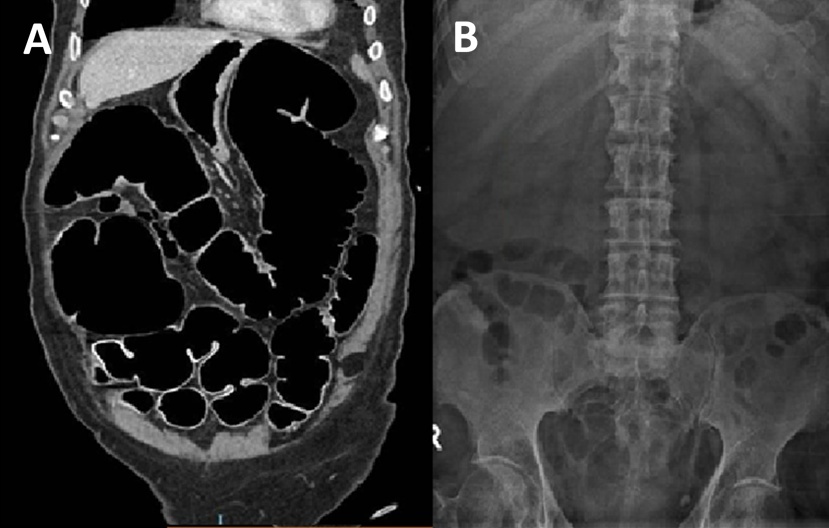
A 75-year-old man admitted to the Neurology Unit for subacute cognitive impairment and ataxia of unknown etiology. During hospitalization, he presented with abdominal distension and constipation associated with fecal vomiting. Abdominal X-ray and CT scans revealed marked colonic dilation without a mechanical cause, suggestive of Ogilvie’s syndrome. After conservative management failed to improve the situation, a decompressive colonoscopy was performed, revealing dilation of the colonic lumen without lesions in any segment. After aspirating gas and fluid, a guidewire was left in place blindly, over which, after removing the endoscope, we advanced a 16-French Salem-type tube under radiological guidance, with its tip positioned in the transverse colon. Initially, we achieved the evacuation of intestinal contents, and after maintaining the tube for a few days with intermittent saline irrigation, the patient’s condition improved (Figure 4).
Discussion
The treatment of colonic decompression via the placement of a fluoroscopically guided transanal decompression tube has been demonstrated to be a safe and effective procedure, regardless of the location or etiology of the obstruction. Furthermore, it helps reduce the recurrence of certain pathologies, such as sigmoid volvulus. It is a simple and cost-effective technique that helps avoid urgent surgical interventions and is useful as a measure prior to elective surgery or the placement of a colonic stent[2]-[5].
The use of a Salem tube with a pre-perforated distal tip placed over a guidewire constitutes an effective alternative for colonic decompression in settings where specific kits are not available, yielding favorable clinical outcomes.