
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Torres Blanco C, Pérez Aisa A, De la Cruz Romero F, Rivas Ruíz F, Pabón Carrasco M, Rodriguez Alonso C et al. First-line eradication regimens in penicillin-allergic patients in Andalusia. Results from the European Registry HP-EuReg in the 2013–2025 period. RAPD 2026;49(3):79-85. DOI: 10.37352/2026493.1
Introduction
Helicobacter pylori (HP) infection affects approximately 50% of the world’s population and plays a key role in the development of chronic gastritis, peptic ulcer disease, mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric cancer.
To date, five consensus meetings on HP infection have been held in Spain, the most recent in May 2021, focusing on the treatment of this infection[1]. The current consensus establishes a higher therapeutic threshold, requiring that empirical regimens achieve, or preferably exceed, a 90% eradication rate according to the intention-to-treat (ITT) analysis.
Thus, in general, a 14-day concomitant quadruple regimen without bismuth (clarithromycin, amoxicillin, metronidazole, and a proton pump inhibitor [PPI]) is recommended for both first- and second-line treatment, or a quadruple combination with bismuth (PPI, bismuth, tetracycline, and metronidazole) for at least 10 days.
In the specific case of patients allergic to penicillin, this same guideline recommends administering the quadruple regimen with bismuth as first-line therapy. To date, available experience with eradication therapies in patients with penicillin allergy is limited, despite the fact that this situation occurs relatively frequently in clinical practice[2]. However, it should be noted that only a small proportion of patients who report a history of penicillin allergy actually have a confirmed immune-mediated hypersensitivity; therefore, it is essential to objectively confirm this diagnosis.
Furthermore, factors influencing the efficacy of eradication therapy must be taken into account, such as treatment adherence, prior history of antibiotic use, and, above all, the prevalence of antibiotic resistance. Numerous studies worldwide have demonstrated an increase in HP resistance over the years. The international multicenter study by Schultz et al.[3] demonstrates that resistance to clarithromycin and levofloxacin exceeds 15% in more than half of the 31 countries included. Meanwhile, amoxicillin showed rates below 2% in most countries.
Another recent study led by the Hp-EuReg (European Registry on the Management of Helicobacter Pylori Infection)[4] found that, in Europe and similarly in Spain, since the 1990s, primary resistance to clarithromycin has fluctuated, remaining consistently above 15%.
On the other hand, resistance to metronidazole has remained high and stable, with prevalence rates exceeding 25%; meanwhile, resistance to levofloxacin has shown a gradual increase, reaching over 19% in recent years.
More specifically in Andalusia, a multicenter study shows that primary HP resistance reaches 18% for clarithromycin and 14% for levofloxacin. Since resistance to clarithromycin exceeds the critical threshold of 15%, guidelines in this region advise against the use of clarithromycin-based triple therapies[5].
Given, on the one hand, the high rate of resistance to clarithromycin and, on the other, the inability to use amoxicillin in patients allergic to penicillin—a drug considered one of the most effective against H. pylori and with low resistance rates—determining the therapeutic approach to H. pylori infection in this patient population poses a genuine clinical challenge.
Objetive
The objective of this study was to analyze trends in treatment regimens for H. pylori infection in treatment-naïve patients with penicillin allergy, evaluating the effectiveness, safety, and adherence to the various regimens used.
Materials and methods
A descriptive observational study was conducted using Hp-EuReg, an international prospective registry focused on the management of HP infection, as the data source. Information was collected using electronic case report forms (e-CRFs) integrated into the AEG-REDCap platform. This is collaborative software developed by the Spanish Association of Gastroenterology and Research Electronic Database Capture, which enables the design, development, and management of electronic data collection forms in research studies, including multicenter studies.
The most frequently used first-line treatments between 2013 and June 2025 were analyzed, including exclusively patients with penicillin allergy. The presence of penicillin allergy was established based on information recorded in the medical records, including both patients with self-reported allergy and those with a previously confirmed diagnosis through evaluation by an Allergy Service. The eleven participating centers were located in the provinces of Malaga, Sevilla, Granada, Almeria, and Cadiz.
Demographic and clinical variables were evaluated, as well as those related to the prescribing, efficacy, and safety of the administered treatments. PPI doses were standardized using omeprazole equivalents and categorized into low-dose (4.5–27 mg omeprazole equivalents/12 h), standard dose (32–40 mg omeprazole equivalents/12 h), and high dose (54–128 mg omeprazole equivalents/12 h). Treatment adherence was defined as taking more than 90% of the prescribed medication. To align the results with routine clinical practice, treatment effectiveness was evaluated using a modified intention-to-treat (mITT) analysis, which includes all patients who completed follow-up and underwent a confirmatory test for eradication success, regardless of treatment adherence.
Descriptive and bivariate statistical analyses were performed, comparing proportions using the chi-square (χ²) and Fisher’s exact tests. Bivariate analysis was used to assess the association between the different treatment regimens and the eradication rate, as well as between treatment effectiveness and the dose of the proton pump inhibitor (PPI) and the duration of treatment. The level of statistical significance was set at p < 0.05. All statistical analyses were performed using IBM SPSS Statistics software, version 28.0 (IBM Corp., Armonk, NY, USA).
Results
During the study period, a total of 5,942 patients were included in the Andalusian registry, of whom 247 (4.2%) were treatment-naïve and allergic to penicillin. Between 2014 and 2017, 51.4% of the total sample was recorded, with 2016 and 2017 being the years with the highest number of patients. The mean age was 54 (+/-14.3; range: 18–84) years, and 70% were women. The most common indication for treatment was dyspepsia (75.3%), followed by peptic ulcer (11.7%), and invasive diagnostic techniques were used in up to 63.2% of patients (Table 1).
Table 1
Socio-demographic and clinical characteristics of the study population.
Overall, the most frequently used treatment was Pylera® (61.8%), a quadruple regimen with bismuth in a single capsule that combines metronidazole, tetracycline, and bismuth subcitrate. In second place were triple regimens (29.7%), with the most commonly used regimens being those combining metronidazole with clarithromycin (18.3%) or clarithromycin with levofloxacin (8.9%). Finally, among the quadruple therapies (8.5%), the regimen based on the combination of metronidazole, doxycycline, and bismuth predominated. Regarding PPI potency, approximately half of the patients received the standard regimen, while high doses were the least commonly used. Furthermore, 10-day regimens were the most commonly used (92.7%) (Table 2).
Table 2
Characteristics of prescribed treatments: treatment regimens used, acid suppression potency of PPIs, and treatment duration.
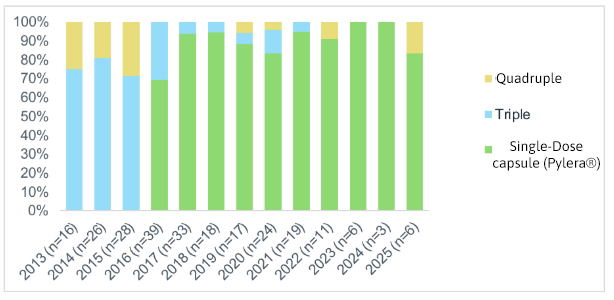
An analysis of treatment patterns over time shows that, at the beginning of the period, triple therapy was the most commonly prescribed regimen. Its use declined significantly starting in 2016, coinciding with the launch of Pylera®, which has since become the predominant option for managing the infection in these patients. Quadruple therapy regimens, on the other hand, have been used to a more limited extent, fluctuating between 28% in 2015 and 17% in 2025 (Figure 1).
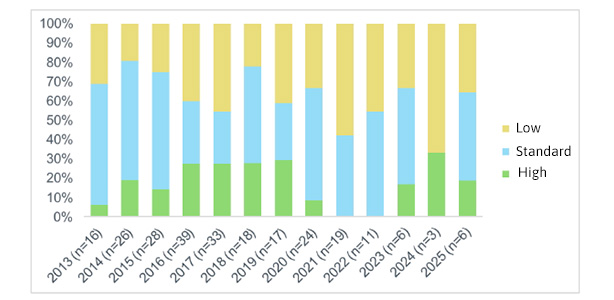
When assessing the potency of the PPIs used throughout the study period, no clearly defined trend is identified. Despite the observed variability, the standard PPI regimen was the most frequently used, while the use of high doses remained the least common option (Figure 2).
Treatment adherence was optimal, estimated at 97.1%, and the overall effectiveness (mITT) of our sample reached 84% (Table 3).
Table 3
Overall therapeutic adherence and effectiveness outcomes.
| Variables | Frequency (n:247) | % | |
| Therapeutic adherence | Yes | 237 | 97.1% |
| No | 7 | 2.9% | |
| mITT | Success | 200 | 84% |
| Failure | 38 | 16% |
When evaluating effectiveness based on the most commonly used treatment regimens (Table 4), it was observed that triple therapies with clarithromycin combined with metronidazole or levofloxacin yielded suboptimal results in patients allergic to penicillin, with eradication rates of 65.1% and 76.1%, respectively. The use of Pylera® in this setting substantially improved outcomes, achieving eradication rates of 93.9%, a statistically significant difference compared with the alternatives (p<0.001).
Table 4
Effectiveness according to the most frequently used treatment regimens.
| Variables | Fracaso | Éxito | p | ||
| n | % | n | % | ||
| Treatment regimen | |||||
| Triple C+M | 15 | 34.9 | 28 | 65.1 | <0.001 |
| Triple C+L | 5 | 23.8 | 16 | 76.2 | |
| Pylera® | 9 | 6.1 | 138 | 93.9 | |
When comparing effectiveness based on PPI dose, eradication rates were similar among the three groups analyzed. In the analysis based on treatment duration, the 10-day regimens showed a higher eradication rate; however, this difference did not reach statistical significance (p = 0.20) (Tabla 5).
Table 5
Effectiveness according to PPI potency and treatment duration.
Finally, adverse effects were reported in approximately 9% of patients, with mild gastrointestinal reactions predominating. The most frequent events were nausea, dysgeusia, and dyspepsia. No serious complications requiring treatment discontinuation were observed.
Discussion
This study demonstrates that, in our setting, treatment of H. pylori infection in penicillin-allergic patients with Pylera® is the treatment regimen of choice. Previously, the most commonly used option was traditional triple therapy with PPI, clarithromycin, and metronidazole, which in older meta-analyses showed eradication rates exceeding 80% [6], but which in more recent Spanish studies has shown a significant decline in effectiveness, with rates below 60%[7][8],. This finding is related to the increase in HP antibiotic resistance[9]-[11]. In fact, the significant increase in resistance to clarithromycin has been global, prompting the WHO in 2017 to include clarithromycin-resistant HP on the list of priority pathogens for new antibiotic research. However, although resistance continues to rise in most countries, it was removed from that priority list in 2024, a decision that has been controversial. Similarly, HP resistance to levofloxacin has also increased in several regions, further complicating the selection of other effective eradication regimens[12]-[21].
With regard to treatment options, recent studies have evaluated combinations such as PPI, tetracycline, and metronidazole in patients allergic to penicillin. These studies have shown ITT eradication rates of 80–85%[22],[23]. The results suggested that this triple combination, or even its quadruple version with the addition of bismuth, could constitute a more effective alternative for first-line treatment in these patients, especially in regions with high resistance to metronidazole or clarithromycin. The efficacy of the quadruple regimen is likely explained by bismuth’s ability to counteract the negative effect of metronidazole resistance[24], which is also administered for an extended period, at short intervals, and in high doses; and because the regimen’s efficacy is not affected by clarithromycin resistance[25]. Furthermore, HP resistance to tetracycline and bismuth is rare[26].
In line with this, a prospective multicenter Spanish study compared the efficacy of triple therapy (PPI, clarithromycin, and metronidazole for 7 days) with quadruple therapy (PPI, bismuth, tetracycline, and metronidazole for 10 days) in 267 patients allergic to penicillin[27]. The results showed an ITT eradication rate of 57% with triple therapy, while the quadruple regimen achieved 74%, confirming the superiority of the latter approach in this population.
In line with this, a recent Hp-EuReg study involving more than 1,000 patients allergic to penicillin showed that the effectiveness of triple therapy as a first-line treatment was only 69%, while quadruple therapy with bismuth, whether in its classic form or via the single-capsule Pylera®, achieved an eradication rate of 91% [28].
All of the above supports the findings of our study, which confirms that Pylera® is not only the most commonly prescribed therapy but also the only one to demonstrate optimal eradication rates. The advantage of using Pylera® as a single-capsule quadruple therapy with bismuth over conventional quadruple therapy with bismuth lies in its more convenient dosing regimen and also overcomes the limited availability of bismuth and tetracycline hydrochloride in many regions. All of this is also in line with the recommendation of the 5th Spanish Consensus on HP Treatment[1].
In our sample, triple therapies were used secondarily, yielding suboptimal results, findings consistent with previously published evidence. Quadruple therapy regimens have had more limited use, and in some years their use was not recorded, although these absences coincided with periods of a lower number of reported cases. In Spain, the use of quadruple therapy with bismuth has been limited mainly by the lack of availability of tetracycline and because doxycycline, although commercially available, has been associated with lower efficacy rates[29].
Therefore, we found a clearly significant association between the therapeutic regimen and effectiveness, favoring Pylera®. However, when analyzing effectiveness based on PPI dose and treatment duration, our results were inconclusive. This finding could be explained, at least in part, by the fact that these variables were evaluated globally, without differentiating among the multiple treatment regimens described. Although not statistically significant, the 10-day treatment duration yielded better results, perhaps largely because it coincides with that of the commercial formulation of Pylera®, the most commonly prescribed treatment.
The main strength of our study is that it is based on a large registry with a long follow-up period, which allows for a detailed analysis of trends in treatment use over time, including a large number of patients and variables. Furthermore, the data is collected from a specific geographic region with common practices in prescribing and managing this clinical scenario. Potential limitations of the study include those arising from the observational nature of the design itself and the existence of periods with fewer recorded data. Furthermore, although the study includes a large sample from eleven centers in five Andalusian provinces (Malaga, Sevilla, Granada, Almeria, and Cadiz), the absence of data from the provinces of Huelva, Cordoba, and Jaen could slightly limit the external validity of the results for the entire Andalusian region. Nevertheless, we believe that the findings obtained are likely to be quite representative of clinical practice in Andalusia.
Conclusion
This study demonstrates a significant shift in treatment patterns for penicillin-allergic treatment-naïve patients in Andalusia between 2013 and 2025, marked by the replacement of triple therapy with quadruple therapy using a single-capsule bismuth formulation (Pylera®) as the predominant regimen following its market launch. This evolution has resulted in excellent outcomes, demonstrating eradication rates exceeding 90%, with optimal adherence and a favorable safety profile, featuring a low incidence of adverse events, most of which were mild.
The findings support the use of Pylera® for 10 days as a first-line strategy in this population with limited therapeutic options, and demonstrate a favorable adaptation of Andalusian clinical practice to scientific evidence, with the consequent optimization of clinical outcomes in this patient group.