
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Bikkuzina-Nasykova A, Parra-López B, Jiménez-Pérez M, Rubio-Herrero Á, Torres-Saavedra M. Gastroduodenal artery embolization outcomes: complications and management. RAPD 2026;49(3):96-99. DOI: 10.37352/2026493.3
Introducción
Upper gastrointestinal bleeding (UGIB) is a common reason for emergency department visits in our region, with an estimated incidence of 48 to 160 cases per 100,000 inhabitants. It accounts for approximately 80% of cases of gastrointestinal bleeding and is the form most frequently associated with serious complications and a greater demand for hospital resources. The most significant risk factors include advanced age, the use of gastrointestinal-damaging drugs (notably nonsteroidal anti-inflammatory drugs), and treatment with anticoagulants, among others. Peptic ulcers are one of the leading causes of upper gastrointestinal bleeding, with duodenal ulcers being the most common. Their clinical significance increases in complicated cases, such as those presenting with significant bleeding, perforation, stricture, or when control cannot be achieved through endoscopic treatment. Other notable causes include complications arising from portal hypertension (PH-associated gastropathy, esophagogastric varices), neoplasms, or vascular anomalies[1].
UGIB is a clinical challenge that often requires urgent intervention. The primary goals of treatment are to stop the acute bleeding episode and prevent rebleeding. Treatment generally requires a multidisciplinary approach with therapeutic options ranging from conservative, endoscopic, or surgical procedures, and sometimes including endovascular techniques [4].
The procedure to be performed will depend on the patient's hemodynamic status and the location of the bleeding. Hemodynamically unstable patients should receive intensive medical care. Once stabilized, they should undergo endoscopy within the first 12 hours. In hemodynamically stable patients, endoscopy may be performed within the first 72 hours following continuous monitoring of vital signs.
If endoscopic therapy is ineffective due to the patient's condition or massive gastrointestinal bleeding, selective catheterization of the bleeding vessel may be necessary via interventional radiology, a technique not without acute and chronic complications, which, in a high percentage of cases, require medical, endoscopic, or even surgical management[2].
Clinical case
We present the case of a 78-year-old man with a history of UGIB due to a duodenal ulcer more than 20 years ago, as well as two subsequent hospitalizations for rebleeding from the same ulcer, manifesting as melena with anemia, in 2024 and 2025.
He was admitted to the Gastroenterology Department for a new episode of upper gastrointestinal bleeding presenting as melena. The patient reported no use of gastrolesive drugs or any new medications. During an upper gastrointestinal endoscopy performed upon admission, a large ulceration was visualized at the duodenal bend with an adherent clot (Forrest IIb), without active bleeding; a nasofibroscope was required to proceed due to marked duodenal stenosis with a significant inflammatory component resulting from the poor healing of the ulcer. Due to the patient's anemia and hemodynamic instability, as well as the impossibility of performing endoscopic treatment, it was decided to perform prophylactic embolization of the gastroduodenal artery.
As no complications were observed following the procedure, he was discharged with close follow-up. One month after discharge, he presented to the emergency department with a febrile syndrome that had been present for approximately 48 hours, as well as hemodynamic instability requiring the initiation of vasoactive medications. He did not present with abdominal pain, jaundice, or any other clinical findings associated with any other condition. Laboratory findings showed elevated acute-phase reactants (CRP, leukocytosis with neutrophilia), anemia with negative urea levels, and an abnormal pancreatic profile. There were no signs of gastrointestinal perforation.
Given the suspicion of an abdominal complication, an abdominal CT scan was performed, revealing inflammatory changes in the duodenum, likely a complicated duodenal ulcer with penetration into the pancreas, as well as a rounded, hypodense lesion within the thickness of the pyloric wall, with parietal thickening of the pylorus, which may correspond to a cystic lesion or abscess. There are no signs of pneumoperitoneum or other collections (Figure 1).
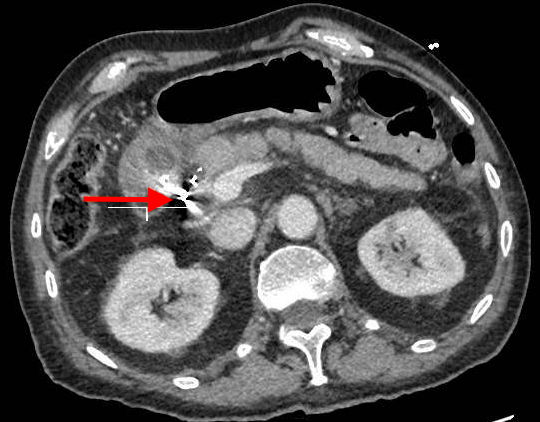
Figura 1
Axial CT scan of the abdomen showing a small ulcer in the duodenum (red arrow), as well as a cystic lesion in the pylorus consistent with a small abscess at that level.
Based on the CT findings, an upper gastrointestinal endoscopy was performed during admission, revealing an inflammatory-appearing stenosis already present prior to embolization, which again prevented the passage of a standard endoscope into the second portion of the duodenum.
Following a review of the case during a medical-surgical conference, surgery was ruled out, and conservative management was therefore initiated, resulting in favorable clinical, laboratory, and radiological outcomes compared to the previous evaluation(Figure 2).
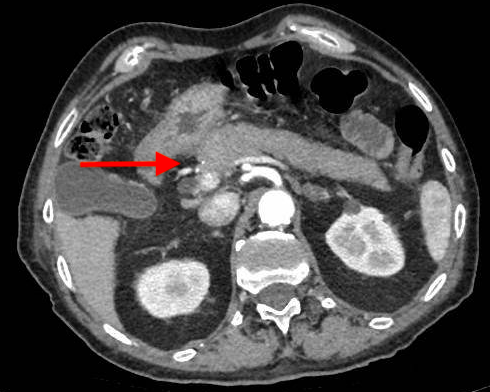
Figura 2
Axial CT scan of the abdomen. Good radiological improvement compared to the previous study, with resolution of the pyloric abscess observed. Known stenosis in the second portion of the duodenum.
At discharge, a follow-up upper endoscopy was ordered to assess endoscopic dilation of the duodenal stenosis. In this examination, a deep ulcer was observed on the posteroinferior wall with partially fibrinous surrounding mucosa, likely related to the penetrating ulcer previously described in imaging studies, with no current active bleeding or other apparent complications. An attempt was made to close the defect with a Hemoclip, but this was not possible due to technical difficulty. Given these findings, a decision is made to readmit the patient for updated imaging studies, and a follow-up abdominal CT scan is performed, revealing a penetrating duodenal ulcer in the second portion of the duodenum associated with retroperitoneal collections, gas, and a thread-like passage of oral contrast from the second portion of the duodenum (Figure 3).
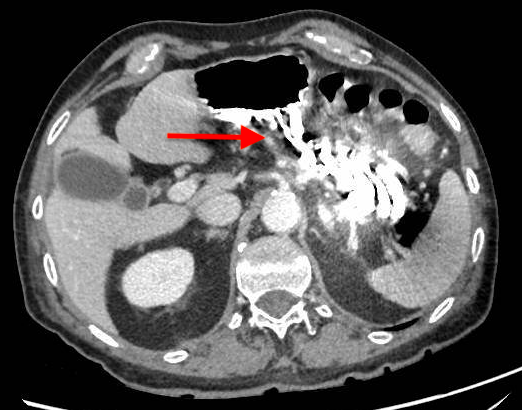
Figura 3
Axial CT scan of the abdomen. A perforating duodenal ulcer is observed in the posteroinferior wall of the second portion of the duodenum, along with encapsulated right retroperitoneal collections containing gas and a thread-like passage of oral contrast from the second portion of the duodenum.
After evaluating all possible treatment options, the patient finally underwent ultrasound-guided percutaneous drainage of the retroperitoneal collection, along with parenteral nutrition and antibiotic therapy. The patient showed favorable clinical and radiological progress (Figure 4). At discharge, the collections had resolved, there was no evidence of oral contrast leakage on the follow-up CT scan, and the patient tolerated a liquid diet well. The patient was discharged due to overall improvement and was scheduled for close follow-up in the gastroenterology outpatient clinic.

Discussion
UGIB is a medical emergency that carries a risk of complications and places a high demand on hospital resources[1].
In certain situations, such as recurrent gastrointestinal bleeding, an unclear source of bleeding, or the impossibility of endoscopic therapy, selective catheterization of the bleeding vascular branch via interventional radiology may be necessary. Compared to surgical procedures, interventional radiological strategies for the treatment of upper gastrointestinal bleeding show similar efficacy in terms of technical success and recurrence rates, but with lower mortality [2].
Arterial embolization in the gastrointestinal tract above the ligament of Treitz is generally considered very safe due to the abundant collateral circulation to the stomach and duodenum. Potential acute post-procedural complications include hematomas at the access site, vascular dissections, contrast-related complications (allergy, nephropathy), or risk of intestinal ischemia [3]. Among chronic complications, duodenal stenosis associated with embolization of the terminal vessels of a bleeding site stands out as a result of severe hypoxia, leading to avascular necrosis[5]. The risk of significant ischemia or stenosis may increase in the presence of additional damage to the collateral circulation due to prior abdominal surgery, radiation therapy, or severe atherosclerosis. In these situations, balloon dilation may be possible, but surgical resection should be considered in refractory cases[3].
As seen in this case, the patient has a history of UGIB due to a duodenal ulcer and frequent rebleeding and was admitted for melena. Gastroduodenal artery embolization was performed following the failure of endoscopic treatment, due to severe inflammatory stenosis present prior to the embolization. One month later, he developed sepsis due to a penetrating duodenal ulcer with pancreatic involvement, which resolved with conservative management.
Therefore, in the presence of acute or chronic post-embolization complications, it is necessary to discuss possible therapeutic solutions in a medical-surgical conference, as medical treatment is a valid and effective option, as demonstrated in this case.