
 Descargar número completo
Descargar número completo Download full issue
Download full issueCORRESPONDENCE
Juan Cristóbal Aguilar Martínez
University Hospital of Jerez
11407 Jerez de la Frontera, Cádiz
CITE THIS WORK
Aguilar Martínez JC, Campos Gonzaga L, Pavón Guerrero MI. Acute emphysematous cholecystitis. An entity to be taken into account in the differential diagnosis of acute abdominal pain. RAPD 2026;49(3):103-105. DOI: 10.37352/2026493.5
Introduction
Acute emphysematous cholecystitis is a rare form of acute cholecystitis with a potentially fatal course, constituting a surgical emergency. Maintaining a high index of suspicion is essential, as it can pose a diagnostic challenge, particularly in its early stages.
Clinical case
A 63-year-old man had no known drug allergies, no history of substance abuse, and well-controlled type 2 diabetes mellitus on oral antidiabetic medications as his only relevant medical history. He presented to the Emergency Department complaining of epigastric and right upper quadrant pain, along with nausea and bilious vomiting that had been present for 24 hours. He reports no fever or other symptoms. He denies any dietary indiscretion prior to the onset of symptoms.
On physical examination, the patient appeared in good general condition, although affected by pain. The only notable finding was tenderness on superficial palpation of the epigastrium and right hypochondrium, with no signs of peritonitis.
Blood tests revealed mild hypertransaminasemia (AST 85 IU/L, ALT 90 IU/L) and mild hyperamylasemia (350 U/L). Acute-phase reactants were not elevated.
Given these findings, the Emergency Department decided to admit the patient to the Gastroenterology ward with a suspected diagnosis of acute biliary pancreatitis.
On his first day in the ward, the patient experienced worsening abdominal pain, which remained unresponsive even to second-line analgesia. Urgent laboratory tests were ordered, but no elevation in acute-phase reactants or other new laboratory abnormalities were detected. Based on the clinical presentation, an urgent abdominal CT scan with intravenous contrast was also ordered, which reported no pathological findings (Figure 1).
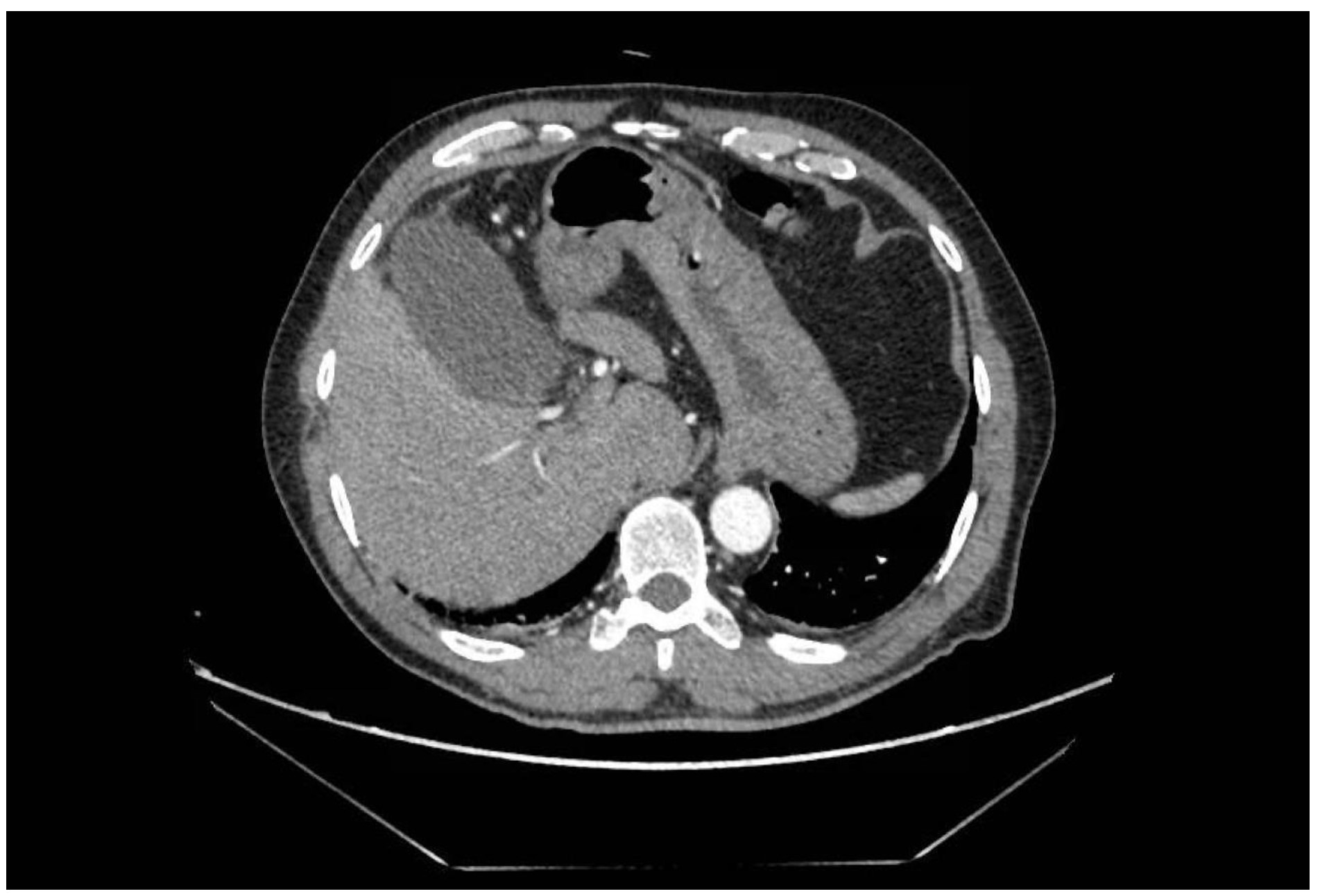
Figure 1
Abdominal CT cross-section with intravenous contrast showing no significant pathological findings in the structures depicted, including the gallbladder.
Just 12 hours later, and given the persistence of symptoms despite analgesia with strong opioids, an urgent abdominal ultrasound was performed. This revealed subhepatic gas, so a new abdominal CT scan with intravenous contrast was performed, showing tomographic findings consistent with acute emphysematous cholecystitis (Figure 2), with gas in the gallbladder wall and subserosal edema. No gallstones or signs of pancreatic pathology were evident in the radiological examinations performed.
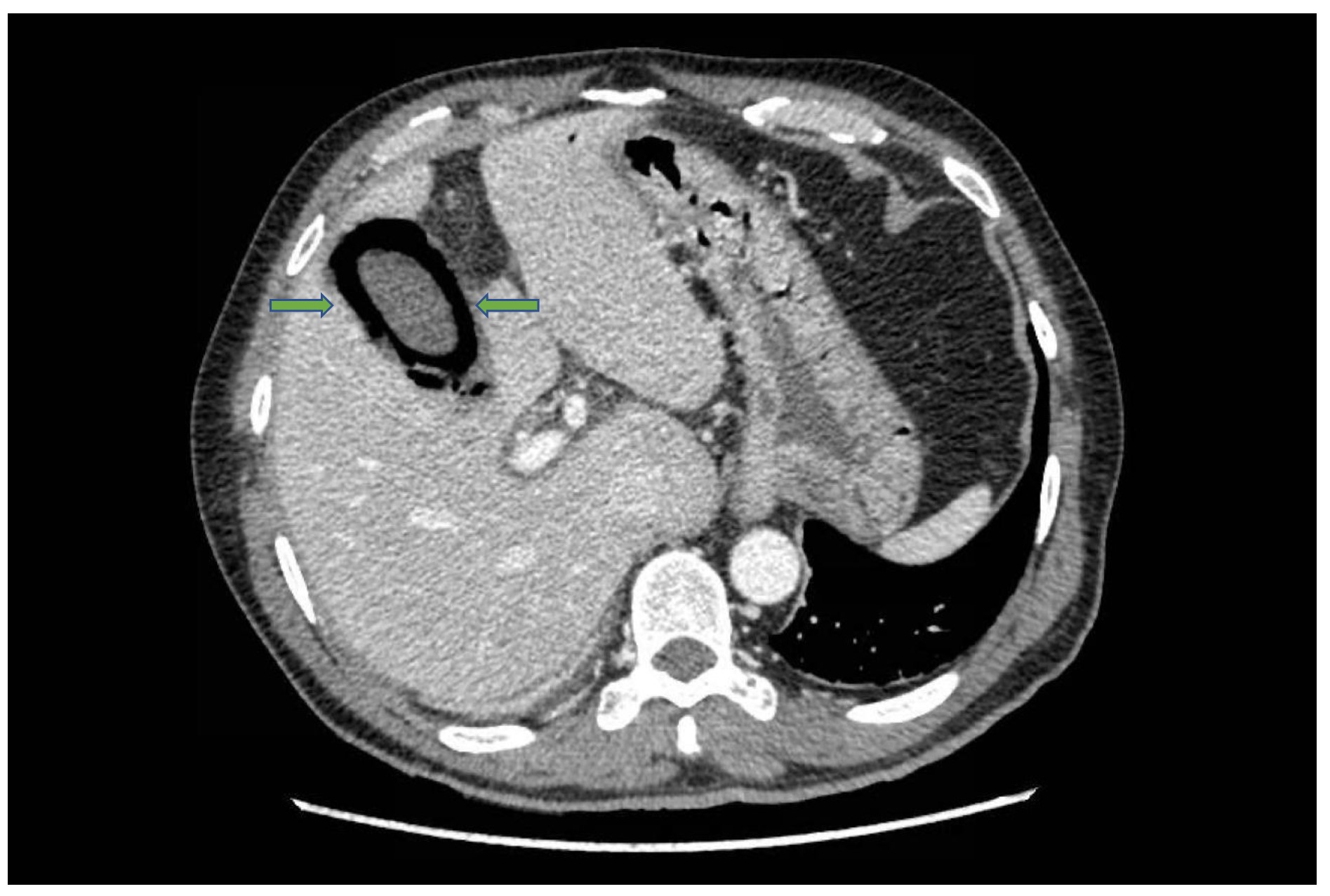
Figure 2
Abdominal CT cross-section with intravenous contrast, performed 12 hours later, showing gas in the gallbladder wall (green arrows), with subserosal edema, consistent with acute emphysematous cholecystitis.
In the absence of significant comorbidities, the case was discussed with the Surgery department. Following their evaluation, broad-spectrum empirical antibiotic therapy was initiated, and an urgent laparoscopic cholecystectomy was performed, with a subsequent favorable outcome. Examination of the surgical specimen confirmed the diagnosis of acute emphysematous cholecystitis, with the isolation of pan-sensitive Clostridium perfringens.
Discussion
Emphysematous cholecystitis is a rare form of acute cholecystitis, accounting for 1% of all cases. Its main distinguishing feature is the presence of gas in the gallbladder wall and/or lumen[1]. The microorganisms most commonly involved are Escherichia coli, Klebsiella spp., and, as in our case, Clostridium spp[2]. It is more common in men, patients with diabetes, and immunocompromised individuals.
Although abdominal ultrasound is usually the first test performed as an initial approach to evaluating abdominal pain, CT is the most sensitive and specific diagnostic technique and is the method of choice. Initially, the clinical presentation is similar to that of acute cholecystitis, but with an insidious and rapidly progressive course toward sepsis and shock, resulting in high morbidity and mortality rates[3].
Therefore, it is crucial to always consider this condition in the differential diagnosis of acute abdominal pain, even when initial diagnostic tests are unremarkable.
Cholecystectomy is the definitive treatment of choice and should be performed as soon as possible. In elderly patients or those with significant comorbidities, echoendoscopy-guided cholecystostomy or percutaneous cholecystostomy may be considered as therapeutic alternatives[4].