
 Descargar número completo
Descargar número completo Download full issue
Download full issueCORRESPONDENCIA
Juan Pedro Toro Ortiz
Hospital Universitario Virgen de la Victoria
29002. Marbella, Málaga
CITA ESTE TRABAJO
Fernández García F, Toro Ortíz JP, Pinazo Bandera JM, Alcántara Benítez R, Ortega Alonso A, Robles Díaz M, Andrade Bellido RJ, García Cortés M. Influence of hepatocarcinoma surveillance programs on cirrhotic patient’s survival: A real life study. RAPD Online. 2022;45(2):44-54.
Introducción
Hepatocellular carcinoma (HCC) is an important cause of morbidity and mortality worldwide, having a decisive influence on the quality of life and vital prognosis of patients with chronic liver disease. HCC is the sixth malignant tumour in incidence and the third in direct mortality[1], presenting a very heterogeneous geographical distribution. The highest incidence rates are located in North Africa and East and Southeast Asia, where the main aetiological factors are aflatoxins and HBV. In Europe, Oceania and America the incidences are lower, the main risk factors being HCV and alcohol, being recently added metabolic associated fatty liver disease (MAFLD)[2]-[4].
Hepatocellular carcinoma settles on a cirrhotic liver in 70-90% of cases[5]. Its prognosis is based on the functional stage of the underlying liver disease and the characteristics of the tumour at the time of diagnosis, with survival ranging from > 70% at 5 years in early stages and < 3 months in advanced stages[6].
Therefore, the early diagnosis of HCC is a primary objective, especially in patients with cirrhotic liver. Accordingly, it is recommended to carry out a diagnostic screening program by means of six-monthly ultrasound scans that allows its detection in early stages, making possible treatments with better survival expectations[7],[8]. The improvement in survival in patients diagnosed with HCC by means of a screening program has been demonstrated. However, the quality and applicability of such screening is variable given that it is limited by the social, health and geographical characteristics of each country and even each health centre[9]-[11].
In our country, this screening is not homogeneous either, since it is not always carried out by personnel with sufficient experience in detecting space-occupying liver lesions; on the other hand, the care overload makes it difficult to respect the time periods between ultrasound scans.
The primary objective of our study was to evaluate the survival rate and the impact of screening on the prognosis of patients with HCC at a tertiary hospital. As secondary objectives, the characteristics of patients were collected, assessing the influence on survival and prognosis of various variables (aetiology of liver disease, comorbidities, age, liver functional stage and tumour staging at the time of HCC diagnosis).
Material and methods
This is a single-centre, retrospective, descriptive and inferential study of patients diagnosed with HCC in a University hospital (Hospital Virgen de la Victoria, Málaga) between January 2012 and May 2018. The patients were identified through the Clinical Documentation Service of our hospital.
Inclusion and exclusion criteria
The inclusion criteria was:
- All HCC diagnosed at our hospital, whatever the stage, between January 2012 and May 2018.
The exclusion criteria were:
- Space occupying hepatic lesions with a final diagnosis other than HCC (including other primary liver cancer, mixed lesions and non-HCC metastasic disease).
- HCC diagnosed outside the period under study.
Clinical and demographical characteristics
Different variables were retrospectively collected: epidemiological, demographic (age, sex), comorbidities (diabetes mellitus, arterial hypertension, HIV co-infection, other active neoplasms or in remission), aetiologies (HCV, HBV, MAFLD, alcohol, autoimmune, toxic, haemochromatosis , mixed or cryptogenic), liver function (Child-Pugh scale), laboratory variables (including alpha-fetoprotein at diagnosis) and clinical variables (ascites, encephalopathy, cirrhosis data and presence of portal hypertension). Regarding the tumour, the diagnostic method (radiological or histological), number and size of lesions were assessed. The condition of the patients was assessed using the ECOG-PS. Then, with the previous data, the BCLC stage was established. Finally, the treatment performed (liver resection, liver transplantation, radiofrequency, alcohol injection, chemoembolization, systemic therapies or best supportive care) and the response to it (remission, recurrence, survival and death), together with survival time, were reviewed.
Abusive alcohol consumption was defined as the intake of more than two standard drinks units in men and one in women. The presence of significant portal hypertension was defined by ultrasound data (portal diameter ≥ 14 mm, splenomegaly), laboratory tests (thrombocytopenia ruled out haematological causes), endoscopic data (presence of esophagogastric varices or portal hypertensive gastropathy) and haemodynamic data (hepatic venous pressure gradient ≥ 10 mmHg). Liver function was assessed using the Child-Pugh classification.
The patients in whom the diagnosis was considered to have been made during screening were those who were followed up in a specialized consultation with six-monthly ultrasound scans and for whom the tumour was first identified in one of these ultrasounds. AFP determination is not included as screening but is often monitored at the follow-up.
We define non-surveillance HCC diagnosis when HCC is detected because of hospitalization, when it is first detected by other radiological techniques or when patients don’t follow the screening properly (for example, one ultrasound per year).
Diagnosis, staging and response to treatment
The diagnosis of HCC was made following the clinical guidelines, where the lesions detected by ultrasound should present typical behavior for HCC on CT or dynamic MRI, that is, hyper-uptake in the arterial phase with lavage in the portal venous phase.8,9 In cases that did not meet these criteria or when the lesions were located on non-cirrhotic livers, a histological diagnosis was made by CT-guided biopsy.
Likewise, information regarding the tumour characteristics at diagnosis was collected according to the BCLC categories: single nodule < 2cm, single nodule ≥ 2 cm and ≤ 3 cm, single nodule > 3cm, up to 3 nodules < 3 cm; multinodular > 3 nodules or 2 or more nodules > 3 cm. Likewise, the presence or absence of extra-hepatic tumour involvement at the time of diagnosis was collected. With all this data, the patients were stratified according to the BCLC classification (0 or very early stage, A or early stage, B or intermediate stage, C or advanced stage, and D or terminal stage).
Regarding the treatment received, the decision was made with the support of a centre-based multidisciplinary Oncology Committee composed of hepatologists and gastroenterologists, surgeons in the hepatobiliary area, medical oncologists and radiotherapists, radiologists and interventional radiologists, specialists in nuclear medicine and pathologists. Patients with an indication for Liver Transplantation (LT) were referred to the reference transplant centre.
Parameters of response to treatment, complications, remission, recurrence, survival and death were collected; in addition to the time in months elapsed.
The response to treatment is assessed following mRECIST criteria:
-Complete response = disappearance of any intratumoural arterial enhancement in all typical intrahepatic target lesions and disappearance of all atypical intrahepatic target lesions and extrahepatic target lesions. Nodal lesions with short axis diameters regressed to -Partial response = at least a 30% decrease in the sum of diameters of the target lesions (including viable tumour diameters for typical intrahepatic target lesions and short axis diameters for nodal lesions), taking as reference the baseline sum of the longest diameters.
- Progressive disease = at least a 20% increase and an absolute increase of at least 5 mm in the sum of diameters of the target lesions (including viable tumour diameters for typical intrahepatic target lesions and short axis diameters for nodal lesions), taking as reference the nadir sum of diameters recorded since baseline.
- Stable disease = neither sufficient decrease to qualify for partial response nor sufficient increase to qualify for progressive disease.
- Not evaluable = at least 1 target lesion is not evaluable and the change in the sum of diameters of the measurable target lesions does not meet the criteria for progressive disease.
Statistical analysis
Statistical analysis was performed with the program SPSS version 23. Categorical variables were expressed as frequencies and percentages, while for continuous variables the mean and standard deviation or the median and interquartile range were used. For the comparison between epidemiological and clinical variables according to the screening group, the Chi-square or t-Student test was used, as appropriate.
The survival study was carried out using the Kaplan-Meier curves and the comparison between curves was assessed using the Mantel-Cox test (log-rank test).
Results
Of a total of 332 patients initially detected together with the Clinical Documentation service, 173 patients were excluded because they presented a final diagnosis other than that of HCC (liver metastases, benign liver tumour, hepatocholangiocarcinoma, cholangiocarcinoma, hepatic lymphoma,) diagnosed before January 2012 or after May 2018 and HCC diagnosed in another centre, resulting in a final sample of 159 patients.
Demographic and clinical characteristics at diagnosis (Table 1).
Table 1
Clinical and demographical characteristics wether underwent HCC surveillance or not. HIV: Human immunodeficiency virus, HCV: Hepatitis C virus , MAFLD: Metabolic associated fatty liver disease, HBV: Hepatitis B virus;. *13 patients (8.1%) were not classifiable by Child-Pugh score (12 non-cirrhotic liver and 1 incomplete diagnosis). **Mixed: 12 cases of HCV and alcohol, 1 HBV and alcohol and 2 cases of HCV, HBV and alcohol simultaneously.
Of the 159 patients included in the study, 130 (81.8%) were male, with a mean age of 67.63 years, somewhat lower in patients diagnosed by the screening program (67.11 years vs 68.78 years), these differences being statistically significant. Regarding the most prevalent comorbidities at diagnosis, 50.3% had arterial hypertension, 34% had Type 2 diabetes mellitus, 3.8% had HIV co-infection, 8.8% had some active extra-hepatic neoplasia and 17.6% had suffered some other neoplasm that was in remission at the time of diagnosis, these data showing no significant differences.
Of the total sample, 147 patients (92.5%) had cirrhosis at diagnosis and 105 (66%) had evidence of portal hypertension. Cirrhotic patients were stratified according to the Child-Pugh classification: 87 patients (54.7%) were in stage A, 43 (27.7%) in stage B and 16 (10.1%) in stage C; 12 patients were not classified as they were not diagnosed with hepatic cirrhosis and 1 due to death before completing the study. When analysing the functional stage in the patients under the screening program, those included in this program were more frequently in early stages (stage A 69%, B 25% and C 2%) compared to those diagnosed outside the program (stage A 32 %, B 32% and C 24%), these differences being statistically significant (p <0.05).
The most frequent aetiology of liver disease was HCV infection (58 patients, 36.4%), followed by alcoholic liver disease (53 patients, 33.3%). However, in patients diagnosed outside the screening program, the most frequent aetiology was alcoholic cirrhosis (39%) and a relevant proportion of cases secondary to MAFLD (11.9%) was also found, resulting in statistically significant differences (p<0.05). The third most frequent aetiology was mixed (15 patients, 9.4%): mainly HCV and alcohol (12 patients), HBV and alcohol (one patient), and HBV and HCV co-infection together with alcohol (2 patients). MAFLD was observed in 11 patients (7%) and in 9 HBV infection as the sole aetiology. Other causes were autoimmune hepatitis, toxic hepatitis and haemochromatosis (one case for each, 0.6%). In 7 patients (4.6%), the aetiology of the liver disease could not be determined as the complete study was not concluded, while in another 3 it could not be established despite thorough diagnostic work-up, so they were considered cryptogenic (1.8%).
Diagnostic methods and characteristics of the tumour (Table 2).
Table 2
Diagnosis, tumor characteristics and HCC staging.BCLC: Barcelona Clinic Liver Cancer.
The diagnosis was radiological in 126 individuals (79.2%) and histological in the rest. Of the total number of diagnosed patients, 100 (62.9%) originated from the screening program.
Regarding tumour size, 12.6% of patients had a single nodule < 2 cm at the time of diagnosis, 13.8% a single nodule ≥ 2 cm and < 3 cm and 38.4% a single nodule ≥ 3 cm. Five percent of patients had 3 nodules or less that were smaller than 3 cm, and 30.2% had multinodular involvement with > 3 nodules or ≥ 2 nodules ≥ 3 cm. Extra-hepatic involvement was detected in 18 patients (11.3%) and portal invasion in 25 (15.7%).
From the point of view of functional status, we found an ECOG 0 in 53.3%, ECOG 1 in 19.5%, ECOG 2 in 11.3%, ECOG 3 in 8.2% and an ECOG 4 in the remaining 7.5%.
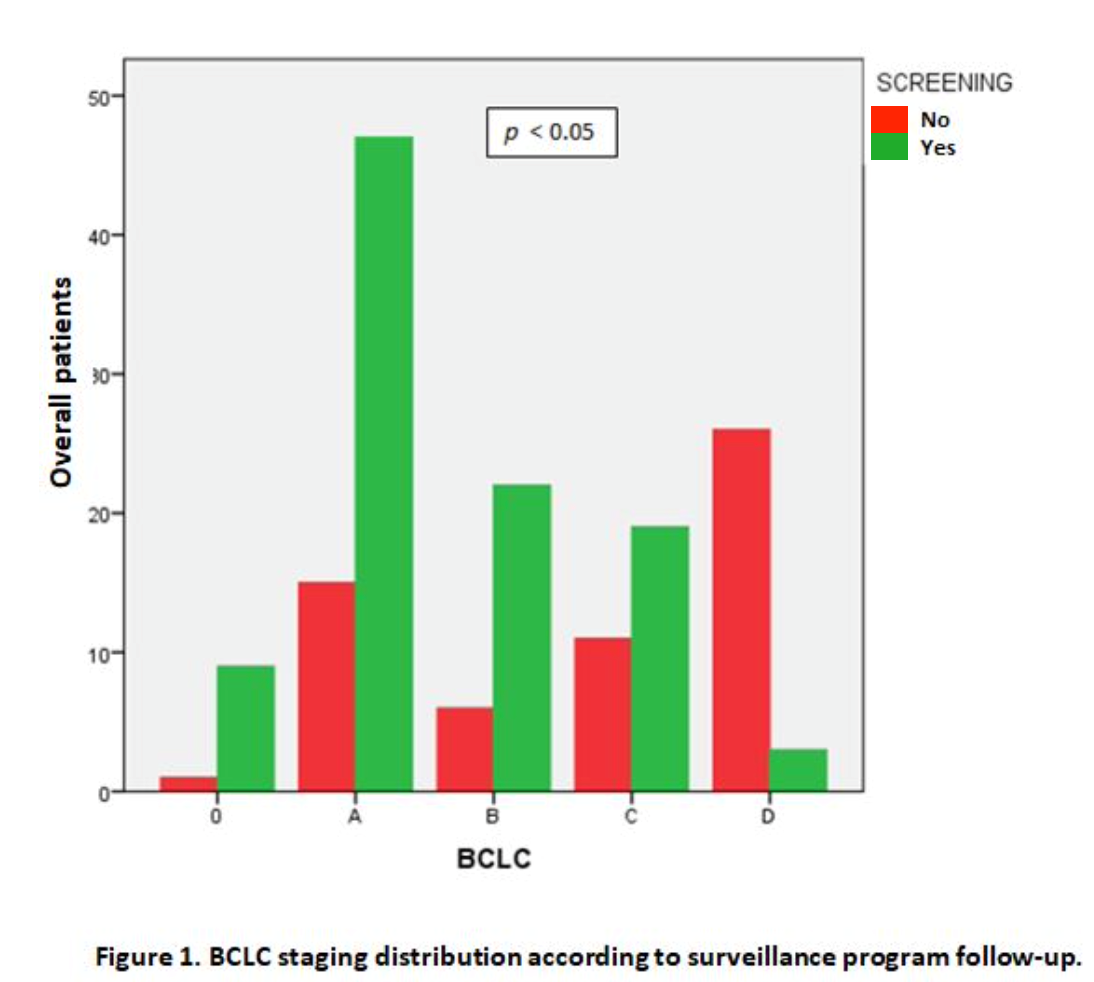
According to the BCLC classification, a predominance of earlier stages was found in patients from the screening program (stage 0 9%, A 47%, B 17%, C 19% and D 3%), data very different from those presented by patients diagnosed outside that program (stage 0 1.7%, A 25.4%, B 10.2%, C 18.6% and D 44.1%), these differences being significant (p <0.05) (Figure 1).
In 127 patients, the AFP level was determined at diagnosis, observing that 106 of these had values above the upper limit of normality (66.6%), with a median of 23.89 and an interquartile range of 273.54, without observing significant differences between patients undergoing screening or not (Table 2).
Therapy (Table 3)
Table 3
Diagnosis, tumor characteristics and HCC staging.BCLC: Barcelona Clinic Liver Cancer.
Eleven patients were referred for liver transplantation (LT): one of them as first treatment, another after failed liver resection and the remaining 9 after previously receiving bridging therapy (4 chemoembolization (TACE), 4 radiofrequency and another combined TACE and RF therapy).
Hepatic resection (HR) was carried out in 21 patients, being the definitive treatment in 11 of them. Of the remaining 10, one was referred for transplantation, another required RF, 2 underwent TACE, 2 received systemic therapy, and the rest required a combination of various therapies.
RF was decided as initial treatment in 28 patients and TACE in 41 (in 9 of them as bridging therapy to transplantation). In 5 patients, the initial treatment was Percutaneous Ethanol Injection (PEI), of which 3 had to be completed with 3 sessions of TACE and in another with more sessions of PEI. During the course of the disease, 2 patients who started treatment with combined RF and/or TACE were subsequently treated with PEI.
Systemic treatment was indicated in 22 individuals (in 10 initially and in 12 at some point in the evolution). The systemic treatment used was Sorafenib in all cases. No other alternative therapies were used.
In 53 patients, symptomatic treatment was initially decided and in 11 more at some point in the evolution.
Overall, those patients who presented a BCLC stage that was favourable and initially eligible for therapies with better survival prospects (HT, RH, RF, and PEI) accounted for 40% of patients from screening versus 20% of those diagnosed outside of screening. In the same way, the patients who were indicated systemic or symptomatic treatment from the diagnosis were 7% and 16% respectively in the group from screening, 5% and 62.7% in patients not screened, these differences being statistically significant (p <0.05) (Table 3).
Regarding the complications recorded, one of the transplanted patients experienced acute rejection and a patient treated by liver resection developed post-surgical pneumoperitoneum that resulted in the death of the patient. As a consequence of TACE treatment, 3 patients developed post-chemoembolization syndrome, while one patient was identified for each of the following complications: fluid retention and ascites, hepatorenal syndrome, mild ischemic hepatitis, and pneumonia with associated pleural effusion. Of the patients treated with Sorafenib, 2 experienced diarrhoea, 1 toxicodermia, and 2 gastrointestinal intolerance.
Evolution and survival (Figure 2)
Figura 2
Survival analysis and sub-analysis. A) Overall survival analysis. B) Survival analysis depending on surveillance program follow-up. C) Survival analysis according to BCLC staging. D) Survival analysis in accordance with first line therapy received
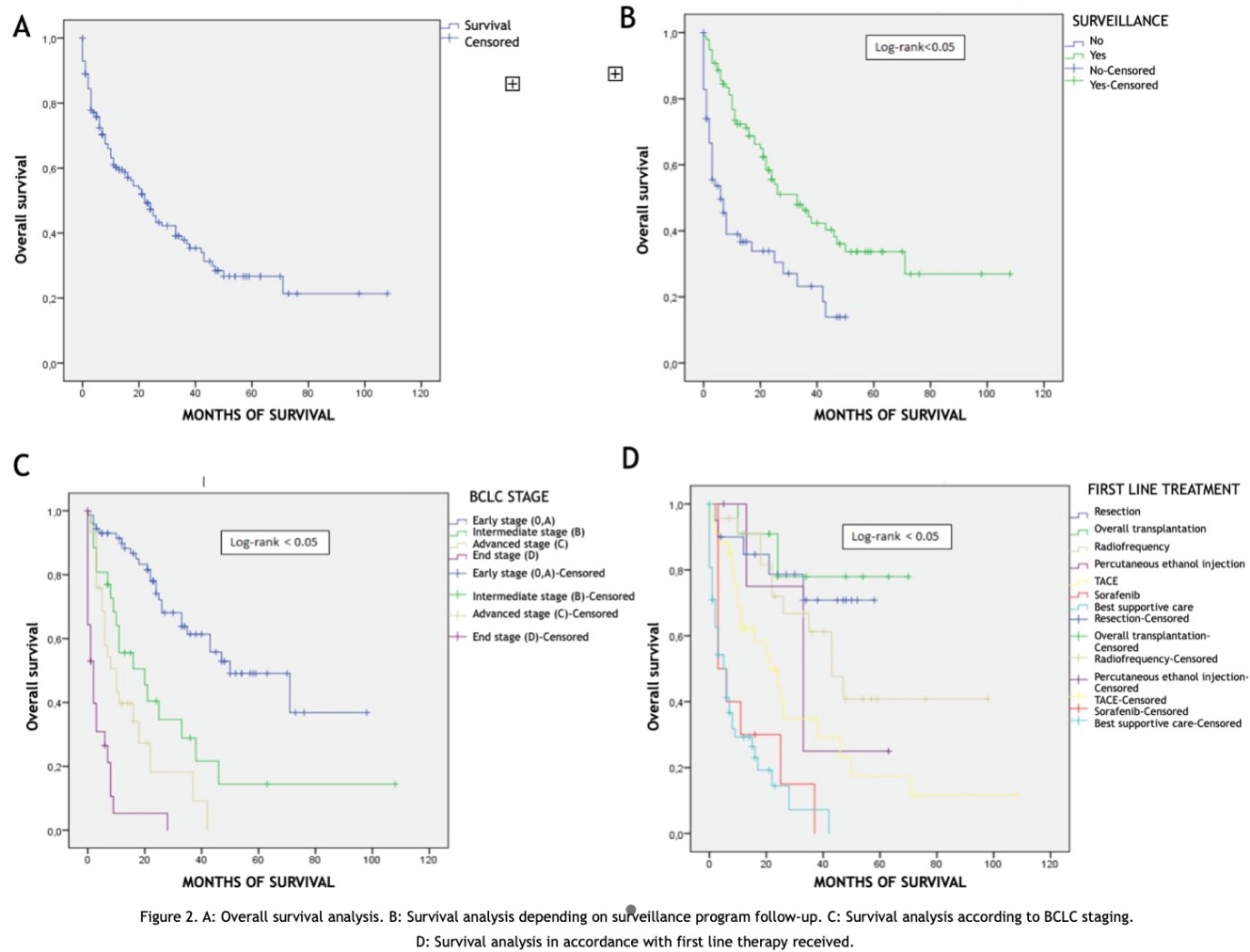
The median follow-up obtained was 13 months (0-108), with loss of this in 4 cases. Of the 59 patients who received treatment with the best survival prospects, 29 (49%) achieved remission, 21 (36%) relapsed, and 9 (15%) had no response. Overall survival was found at 1, 2, 3 and 4 years of 60.3%, 47.3%, 37% and 27% respectively with a median survival of 22 months (95% CI 16.11-27.89) (Figure 2).
Evaluating the results according to the origin or not of the screening program, it was found that the patients coming from it had a median overall survival of 33 months (95% CI 20.25 - 45. 74) and a cumulative survival at 1, 2, 3 and 4 years of 72.3%, 55.5%, 44.2%, 34% versus an overall survival of 6 months (95% CI 1.97 - 10.02) and a cumulative survival of 1, 2, 3 and 4 of 36.7%, 30%, 22% and 0% in those diagnosed outside the program, this comparison being statistically significant (p <0.05)(Figure 2).
We performed a survival analysis based on tumour stage (BCLC classification at diagnosis). Survival was calculated by merging stage 0 and A for stability of the analysis; finding statistically significant differences when comparing these curves (Figure 2): a median of 50 months (95% CI 27.64-72.35) for early stage (0 and A), 20 months (95% CI 6.49 - 33.55) for stage B , 10 months (95% CI 4.91 - 15.08) for stage C and 2 months (95% CI 0.44 - 3.55) for stage D.
Survival analysis was performed based on demographic and tumour characteristics at diagnosis, some of these, in turn, forming part of the BCLC staging system. Regarding the characteristics of the tumour lesion, a median survival of 43 months (95% CI 20.41 - 65.58) was found for single nodules ≤ 3 cm, 24 months (95% CI 15.59 - 32.40) for single nodules > 3 cm, 22 months (95% CI 0 - 58.61) for lesions with less than 3 nodules and these < 3 cm and 9 months (4.98 - 13.01) for lesions with more than 3 nodules or these > 3 cm; the difference between these survival curves being statistically significant (p log-rank <0.05).
The survival related to the functional stage (Child-Pugh classification) was similar at diagnosis, with the median for stage A being 35 months (95% CI 21.43 - 48.56), stage B 10 months (95% CI 0 - 20.74) and 2 months stage C (0 - 6.75). Survival in patients with portal hypertension was significantly lower (median 16 months, 95% CI 7.55 - 24. 45) versus those who did not present it (median 46 months, 95% CI 31.60-60.39). Likewise, patients with portal tumour invasion at diagnosis showed a lower survival than the rest (median 3 months, 95% CI 0.72 - 5.27 vs 26 months, 95% CI 17.06 - 34.93). The comparison of the survival curves according to the ECOG classification also showed statistically significant differences with a median of 50 months (95% CI 27.41 - 72.59) for stage 0, 24 for stage 1 (95% CI 18.85 - 29.15), 6 for 2 (95% CI 1.81 - 10.18), 5 for 3 (95% CI 0 - 10.36) and 0 for 4.
Finally, the median survival rates obtained in our series, according to the initial treatment, were the following (Figure 2): 58 months (95% CI 44.43 - 72.71) in transplant patients (with bridge therapy or not), 45 months (95% CI 36.53 - 55. 08) for HR, 43 months (95% CI 29.2 - 56.79) in those treated with RF, 33 months (95% CI 16. 02-49.97) with PEI, 21 months (95% CI 9.84 - 32.15) for TACE, 12.5 months (95% CI 3.96 - 21.03) for systemic therapy and 5 months (95% CI 2.37 - 7.62) in the best supportive care treatment group ; the difference between the curves being statistically significant (p log-rank <0.05).
No statistically significant differences were found in survival based on the other epidemiological, clinical and diagnosis-related characteristics.
Discussion
The high incidence and mortality of HCC is a growing challenge for healthcare systems across the world. A screening program has been devised in patients with cirrhosis based on six-monthly ultrasound scans, with the aim of achieving an early diagnosis and reducing mortality from this disease. Numerous studies have assessed the efficacy of such screening in cirrhosis[12]-[14].
Despite the recommendation to carry out a screening program, it has been estimated that <20% of patients with cirrhosis undergo follow-up. On the other hand, it is estimated that in patients who are regularly followed up in a speciality clinic, adherence to the screening program is slightly higher than 52%[14]-[16]. In our series, of the 159 patients diagnosed with HCC, 62.9% were included in the screening program, these figures being higher than some published series. The causes that make it difficult to apply screening to a higher percentage of patients can be attributed to multiple failures. Fasiha Kanwal and Amit G Singal describe several of these causes, highlighting the difficulty of the healthcare system in making an early diagnosis of liver disease (pre-cirrhotic phase) and the importance of achieving adherence to said screening, recommending favouring travel and strengthening follow-up during the first year to create a habit in the patient[17].
In our series, no epidemiological characteristics showed significant differences between the two groups (under screening or not), identifying the mean age of the patients diagnosed under the screening program as younger compared to the other group (67.11 years vs 68.78 years); data consistent with those described in other series[18],[19].
The most frequent aetiology in our sample was HCV, followed by alcohol, in both groups, similar to the results from Western countries[20],[21] An overrepresentation of patients with MAFLD aetiology in the non-screening group was noticeable. Probably the slow and silent evolution from steatosis to steatohepatitis and fibrosis can explain this fact;[21],[22] this makes it difficult for patients to be aware of their disease, not consulting, and early diagnosis and follow-up is not feasible.
Although in the different studies there is no unanimity of results regarding the screening of HCC[23], the clinical practice guidelines of the Asian, American, European and Spanish societies, as well as several recent studies support its implementation It achieves the identification of tumour lesions in smaller numbers and sizes and with less tendency to extra-hepatic involvement, that is, in less advanced stages[8],[24]-[26]. In a recent publication which evaluated the efficacy of screening in a sample of more than 13,000 patients diagnosed with HCC between 2003 and 2013, Choi et al showed that between 42.4% and 63.6% of the screened patients were diagnosed with HCC that met the Milan criteria, while in those not screened, only 25.3% fell within these criteria[27]. In our series we found similar results, identifying HCC in earlier functional stages in patients under a screening program, less presence of portal invasion at diagnosis and better functional situation, all of which is summarized in a better BCLC stage in patients from screening compared to those who did not follow it (see Table 1), all these results being statistically significant (p <0.05).
The immediate and most relevant consequence of making diagnoses in earlier stages is the possibility of offering potentially curative treatments, with the aim of reducing disease-related mortality and increasing survival[28],[29].Therefore, it would be expected that screening would have a direct impact on the overall survival of these patients. The survival rate can be highly variable as shown in the literature. The multi-centre and international observational study HCC BRIDGE showed a great difference in the median survival rates between the different regions: 60, 33, 31, 24 and 23 months for Japan, the United States, South Korea, Europe and China respectively[30].In our series we found a median overall survival of 22 months (95% CI 16.11-27.89), similar to that observed in other studies carried out in our environment[31],[32].
Regarding the relationship between screening and survival, recent studies and meta-analysis[12],[27] show the benefit of achieving an early diagnosis through screening, although other series do not confirm this evidence[23]. This disagreement could be due to the incorrect application of screening in clinical practice[33].
In addition to screening, many other factors can influence the prognosis of these patients, such as tumour stage at diagnosis (BCLC). Survival without treatment is estimated to be > 36 months in stage 0, < 36 months in stage A, 16 months in stage B, 4-8 months in stage C, and < 3 months in stage D[8],[34].In our series, survival (see figure 2) was with a median of 50 months for early stage (0 and A), 20 months for stage B, 10 months for stage C and 2 months for stage D, these data being similar to those of international series[30],[35].
Analyzing other prognostic factors, it was evidenced that the number and size of tumour lesions, the functional stage according to Child-Pugh, the presence of portal hypertension or portal tumour invasion determined significant differences in terms of survival, these facts being widely confirmed in the literature[6],[8],[36],[38].
The objective of HCC treatment is to extend survival with the best possible quality of life, with different useful therapies depending on the tumour stage (BCLC)[28]. Liver transplantation would be the ideal treatment when conditions permit, with > 70% survival at 5 years. Liver resection achieves a survival rate of 50% and 72% at 5 and 3 years, respectively. Similar efficacy is obtained with RF when used in nodules < 2 cm[8],[34],[37],[38].TACE, according to certain series, could reach a median survival of 30-40 months if performed in selected patients[39]-[41].Systemic treatments have been a revolution in recent years, with new drugs appearing both in the first line (Sorafenib, lenvatinib or the combination of atezolizumab and bevacizumab) and in the second line (regorafenib, cabozantinib or ramucirumab) with the aim of increasing survival[42], obtaining survivals in the first line of 10-13 months, and less than 10 months for the second[26].
These data are comparable with the data obtained in our study, where the survival results (see figure 2) obtained according to the initial treatment have been 58 months in transplant patients (with bridge therapy or not), 45 months for RH, 43 months for those treated with RF, 33 months with PEI, 21 months for TACE , 12.5 months for systemic therapy and 5 months in the best supportive care treatment group; the difference between the curves being statistically significant (p log-rank < 0.05).
The limitations of our study should be noted, which mainly reside in its retrospective design.
In conclusion, the data from our study in routine clinical practice, further support that the screening program achieves a diagnosis of HCC in earlier stages, favouring the use of potentially curative treatments and, therefore, improving the overall survival of these patients.
Authors’ contributions
Made substantial contributions to conception and design of the study and performed data analysis and interpretation: Toro JP, Fernandez-Garcia F, García-Cortes M, Alcantara R; performed data acquisition, as well as provided administrative, technical, and material support: Fernández-García F; Toro Ortiz, JP, Pinazo-Bandera J; Alcántara R; Ortega-Alonso A, Garcia-Escaño MD, Robles-Diaz M; García-Cortés, M; Critical revision of the manuscript: Andrade J, Alcantara R, Garcia-Cortes M.