
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITATION
García Martínez A, Mateos Millán D, Morales Prado Á, Prieto García JL. Bouveret's syndrome and digestive endoscopy as diagnostic support. RAPD 2024;47(1):37-39. DOI: 10.37352/2024471.4
Introduction
Bouveret's syndrome is a rare form of biliary ileus that involves the passage of a large lithiasis (usually larger than 2 cm) from the gallbladder into the intestinal lumen through a cholecystoduodenal fistula, causing obstruction to the gastric outflow or the proximal intestine. It was first described in 1896 by Léon Bouveret (Lyon, France)[1]-[3].
Clinical Case
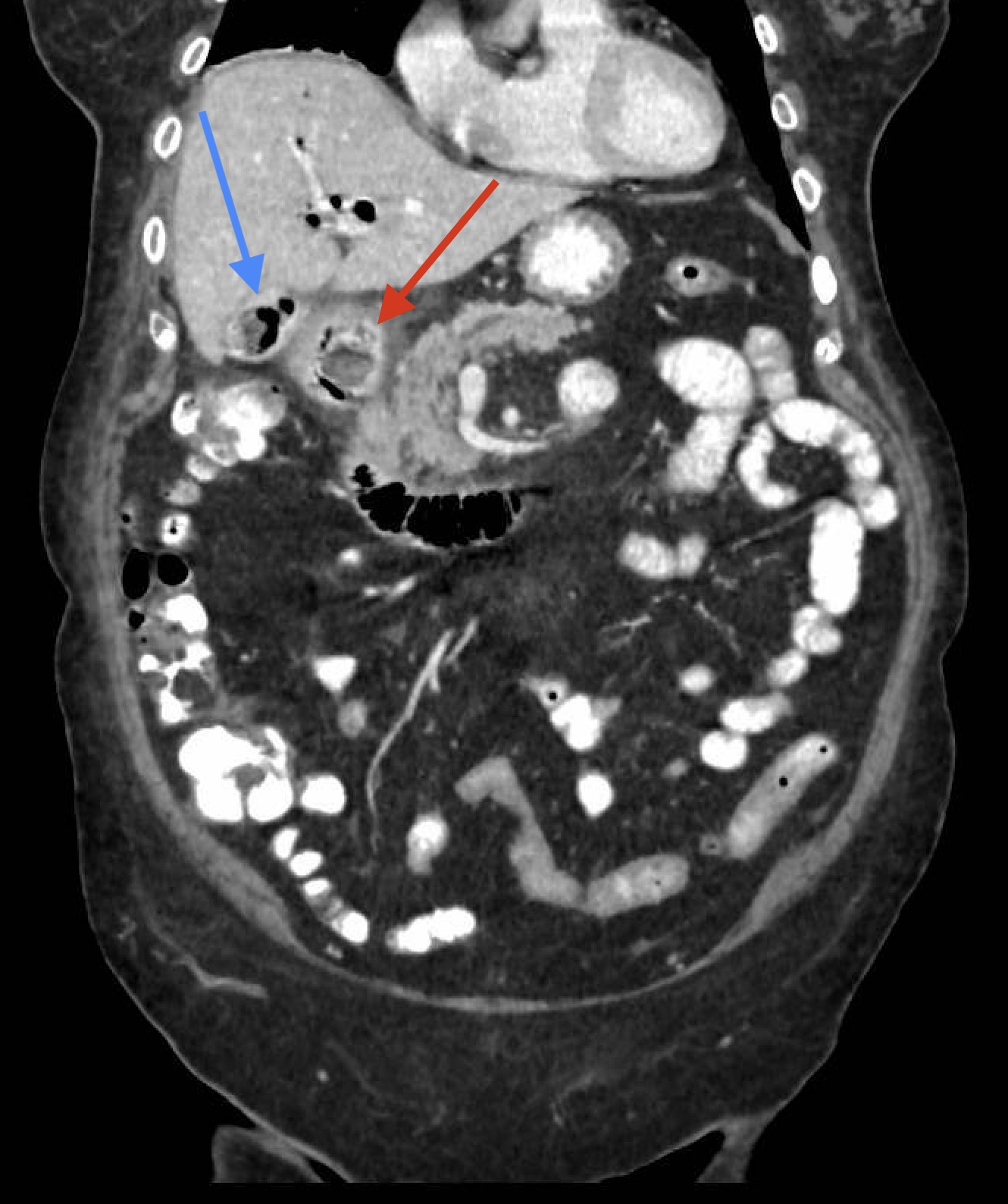
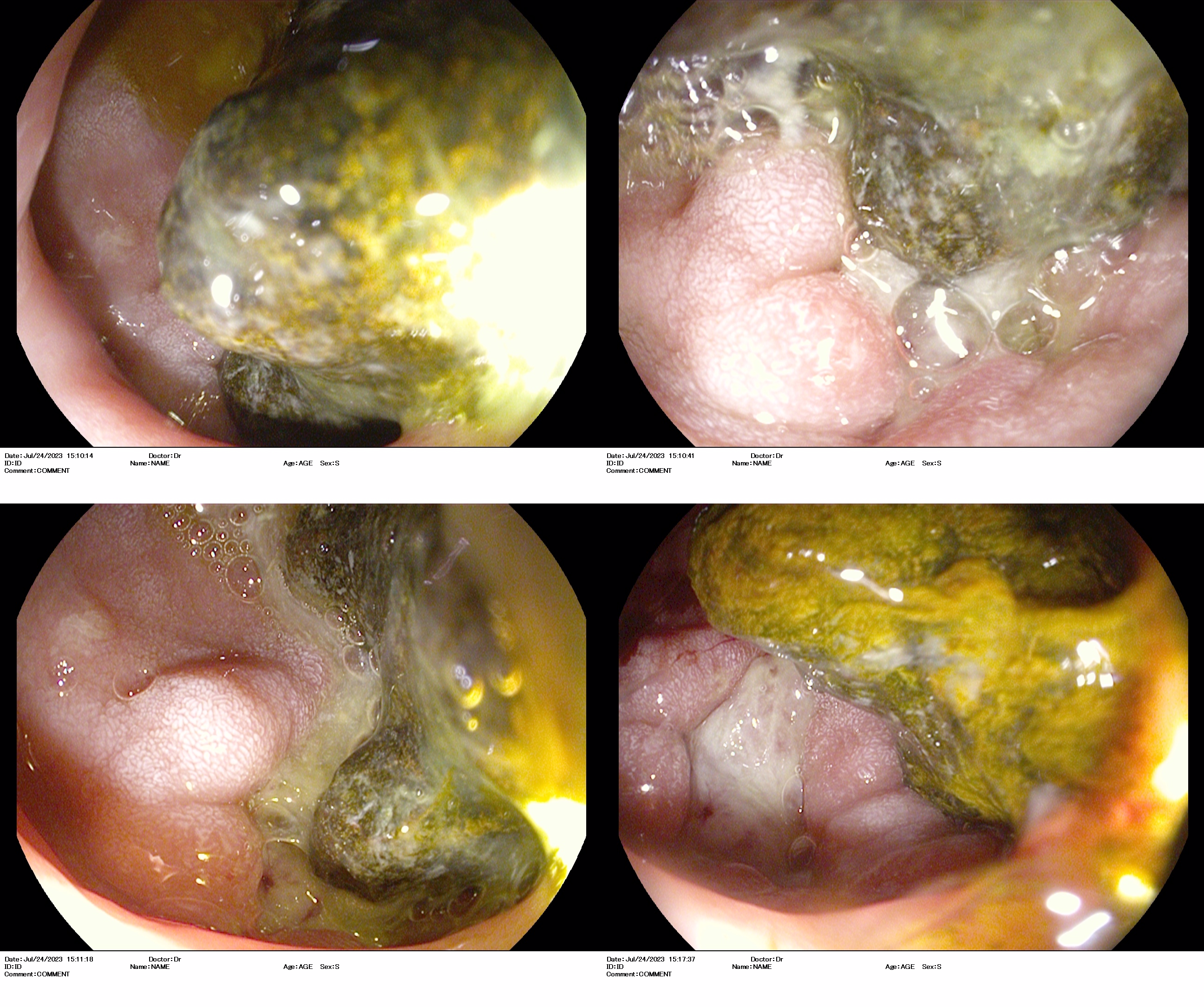
This is an 80-year-old woman with a history of cholelithiasis who was admitted to hospital for epigastralgia, postprandial fullness feeling and vomiting. Once hospitalised, a further study was performed with cholangioresonance imaging and abdominal tomography (Figure 1), which identified an oval lesion occupying the duodenal bulb, as well as aerobilia and air in the gallbladder together with the known lithiasis. In view of these findings, an oral endoscopy was requested, confirming a fistula and an oval lithiasis of approximately 30 mm in the duodenal bulb (Figure 2), which prevented passage to the second portion of the duodenum. Endoscopic fragmentation was attempted with all available instruments (loop, biopsy forceps, tripod, etc.) and even direct extraction without success. Subsequently, the patient was evaluated with an advanced endoscopy unit of reference (given that we do not have endoscopic retrograde cholangiopancreatography in our centre) to assess electrohydraulic lithotripsy, but this was rejected due to unsatisfactory results in other patients with similar characteristics as well as the current evidence in this regard. Therefore, she was assessed by the surgical team and scheduled surgical extraction of the stone was performed with an acceptable subsequent evolution.
Discussion
This syndrome usually occurs in women over 70-75 years of age with comorbidity and its clinical presentation consists of a high intestinal obstruction (gastric distension that improves with vomiting, frequent and abundant vomiting, as well as epigastric or right hypochondrium pain)[3],[4].Pathophysiologically, the formation of the fistula between the gallbladder and the lumen of the digestive tract is due to a chronic inflammatory reaction, which stops the free perforation and allows the passage of the lithiasis. However, only 6% of lithiasis that pass into the digestive tract result in intestinal obstruction due to size, occurring mainly in the terminal ileum (50-90%), proximal ileum and jejunum (20-40%) as well as the duodenum (less than 5% of cases)[5].
Clinical suspicion is essential for diagnosis, although a summary is made on the basis of clinical, radiological and endoscopic factors. Plain abdominal X-ray may show Rigler's triad (small bowel obstruction, pneumobilia and ectopic lithiasis) but is present in only one third of cases[2],[3],[5]. Ultrasound of the abdomen is useful to exclude acute cholecystitis. CT scan is diagnostic in 60% of cases, which can be complemented by magnetic resonance cholangiopancreatography, since 15-25% of cholelithiasis are isodense. Finally, endoscopy supports the diagnosis as it allows direct visualisation of the lithiasis (up to 70% of the time), the orifice of the duodenal fistula and to rule out other differential diagnoses (such as neoplasms)[3]-[5].
Regarding treatment, both endoscopic and percutaneous treatment options have been described, including retrieval basket or polypectomy loop and fragmentation methods with mechanical lithotripsy, laser, extracorporeal shock wave and intracorporeal hydraulics[3],[4],[6]. Given the advanced age and comorbidity that patients with Bouveret's syndrome often present, endoscopic removal should be attempted in the first instance[4]. However, the overall success rate with endoscopic procedures is only 37-43% and in many cases all endoscopic alternatives fail, especially in cases of large (> 2-3 cm) impacted lithiasis[4],[7]. Cappel et al. have reported a therapeutic success rate with YAG-laser lithotripsy of 60% and only 25% and 20% for mechanical lithotripsy and extracorporeal shock wave lithotripsy, respectively[8]. On the other hand, cases have been described of Bouveret's syndrome complicated by distal small bowel obstruction due to impaction of part of the original previously fragmented lithiasis, whose removal required a new endoscopic procedure or, more frequently, surgical treatment[4].Therefore, up to 91% of cases will require surgery due to failure of these therapies, consisting of lithiasis removal as well as fistula repair, with a success rate of more than 80%[3],[4].Cholecystectomy is usually optional but mandatory in case of intravesicular lithiasis[3],[4],[9].Due to the age and comorbidity of the patients, Bouveret's syndrome has a morbidity of 60% and a mortality of 12-30%[3].
In conclusion, this is a pathology that requires close collaboration between endoscopists and surgeons. Although there are no standardised protocols for the management of these patients, endoscopy is diagnostically useful and potentially therapeutic. In case of large impacted lithiasis, endoscopists should be prepared to use multiple endoscopic instruments including lithotripsy to maximise success rates. In case of failure of endoscopic treatment, lack of experience or unavailability, a surgical option would be justified[6].