
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Grilo Bensusan I, Torres Gómez J. Microscopic colitis. RAPD 2025;48(1):51-58. DOI: 10.37352/2025482.2
Introduction
Microscopic colitis (MC) is an inflammatory disease affecting the large intestine that includes collagenous colitis (CC), lymphocytic colitis (LC) and recently incomplete forms of the same: incomplete MC[1]. Its diagnosis is based mainly on histological findings obtained by studying colonic biopsies in patients with persistent watery diarrhea. It is a pathology whose incidence has increased in recent years, equating in some regions to inflammatory bowel disease. The involvement and collaboration of the gastroenterologist and the pathologist are important for an adequate diagnosis of the patient.
Definition
MC, according to the recommendations of the Spanish MC group, is a generic term that includes LC and CC. It refers to an inflammatory bowel disease characterized by the existence of chronic or intermittent diarrhea, without blood in the stool, with macroscopic findings on colonoscopy that are normal or near normal and that present defined histological features[2]. When these histological features are not completely fulfilled in patients with compatible symptoms, the term incomplete MC has been coined[3].
Epidemiology
CC was first described more than four decades ago in 1976 by Lindstrom. The term MC was introduced by Read et al. in 1980 and finally Lanzeby introduced the term LC[4]. Today, the term MC includes CC, LC and incomplete MC[1].
The incidence of MC globally is estimated at 11.4 cases per 100,000 inhab/year[3]. There are differences between countries ranging from 6.8 to 24.7 per 100,000 inhabitants/year.[1]. With respect to CC, in Northern Europe and North America it varies between 5.2 and 10.8 cases per 100,000 inhabitants/year, being lower in Spain at less than 2.9 cases per 100,000 inhabitants/year. LC is more frequent, with an incidence in Northern Europe and North America of 4 to 19 cases per 100,000 inhabitants/year and in Spain of 2.3 to 16 cases per 100,000 inhabitants/year[2]. Its incidence has been increasing in recent decades, although it seems to have reached stable levels since the 2010s[1]. This increase has caused its incidence to match that of inflammatory bowel disease and in some countries to exceed the incidence of Crohn's disease[5],[6]. The increased incidence is attributed to increased access to colonoscopy, increased suspicion and awareness on the part of gastroenterologists and pathologists, and increased exposure to risk factors, but none of these aspects have been confirmed by studies designed for this purpose.[1],[6].
The incidence is 2 to 8 times higher in women than in men. This difference is greater the older the age at diagnosis and is higher in CC than in lymphocytic [1]-[3].
The risk of developing MC increases with age, with a peak incidence occurring in the seventh decade of life with a mean age at diagnosis of CC of 64.9 years and 62.2 years in LC, between 61.1 +/- 6.5 years in MC overall [2],[7]. However, up to 25% of cases occur in children under 45 years of age and cases have also been reported in children[2].
The estimated prevalence of MC is 119 cases/100,000 population, being 50.1 per 100,000 population for CC and 61.7 per 100,000 population for LC[3].
Pathogenesis
The pathogenesis of MC is unknown. The most accepted hypothesis is the existence of an inadequate immune response, in response to stimuli of the colonic mucosa, in genetically susceptible individuals. This response provokes an inflammation of the mucosa that gives rise to the fundamental symptom of the disease, which is diarrhea[1],[6] (Figure 1).

Regarding the immune response, the infiltrate observed in the lamina propria in MC is formed by cytotoxic CD8 lymphocytes and CD4 helper lymphocytes. Their presence causes an increase in cytokines, interleukins, tumor necrosis factor and interferon gamma that act as proinflammatory factors. Collagen formation is associated with an imbalance in its production and destruction process, associated with increased expression of tumor growth factor beta(TGF-β). (1,6) This inflammatory response causes an increase in intestinal permeability, mediated by IFN-gamma and TGF-β and associated with a decrease in claudins, proteins responsible for the intercellular junctions of the colonic epithelium[1].
The triggers of this inappropriate immune response are unknown. They primarily involve exposure to bacterial products, drugs or other chemicals. In relation to bacteria, a recent Danish study associates the incidence of MC with enteric infections by Campylobacter jejuni and Campylobacter concisus, without association with infection by Salmonella spp. The microbiota is also implicated in the pathogenesis of the disease based on its improvement when fecal flow is diverted by ileostomy, or the appearance or improvement of the picture when a fecal transplant is performed. Some noteworthy findings in the microbiota of patients with MC are the existence of a dysbiosis with a reduction in species diversity. Among them, a reduction in the family Ruminococcaceae, Collinsela, Coriobacteriaceae, Clostridiales, Akkermansia and Alistipes is observed. However, further studies are needed to corroborate these findings[1]. Drugs that are associated with an increased risk of MC are proton pump inhibitors (PPIs), non-steroidal anti-inflammatory drugs (NSAIDs) and selective serotonin reuptake inhibitors (SSRIs)(Tabla 1). However, this association does not imply their causal relationship. Chronic use of PPIs significantly increases the risk of CM with an OR of 2.95 (95% CI: 1.82-4.8). This risk is higher for CC. The proposed mechanism for this increased risk appears to be related to modification of intestinal permeability and intestinal microbiota. NSAIDs also increase the risk of MC with an OR of 2.4 (95% CI: 1.99-2.89). Concomitant use of PPIs and NSAIDs could further increase the risk. Finally, SSRIs also increase the risk with an OR of 2.98 (95% CI, 2.35-3.78). The mechanisms by which NSAIDs and SSRIs favor the development of MC are not known. Other drugs that may increase the risk are hormone replacement therapy in women, with a higher risk associated with a longer treatment time. Oncological immunotherapy also produces enterocolitis, which in some cases meets the histological criteria for MC. In these cases there is a response to budesonide and they have a better prognosis than other forms of enterocolitis caused by these drugs. Less evidence of their implication in the development of CM has ticlopidine, beta-blockers, angiotensin converting enzyme inhibitors (ACE inhibitors), angiotensin 2 receptor antagonists (ARA-2), oral antidiabetics and statins[1],[3].
Smoking is another factor that increases the risk of developing MC. A history of smoking increases the risk with an OR of 1.6 (95% CI, 1.4-1.9), whereas active smoking increases the risk with an OR of 2.99 (95% CI, 2.15-4.15), being higher for CC (OR: 5.5, 95% CI: 3.4-8.9). The mechanism implicated is alteration of the intestinal barrier, alteration of humoral and cellular immunity, alteration of the intestinal microbiota and stimulation of fibrogenesis by TGF-β stimulation[1],[3].
A lower body mass index could increase the risk of MC. There are no conclusive data regarding the consumption of alcoholic beverages[1].
Finally, from the genetic point of view, haplotypes of the HLA complex have been detected that increase the risk of developing MC. Specifically, the ancestral haplotype HLA 8.1 is associated with CC, although not with LC. CC has also been associated with more frequent alleles in Crohn's disease and ulcerative colitis. It has also been associated with alterations in chromosome 6 (HLA DQ2) associated with celiac disease[1],[6].
Table 1
Drugs associated with an increased risk of MC. PPIs: Proton pump inhibitors. NSAIDs: non-steroidal anti-inflammatory drugs. SSRIs: selective serotonin reuptake inhibitors. ARA-2: Angiotensin II receptor antagonists.
El tabaquismo es otro factor que aumenta el riesgo para padecer una CM. El antecedente de consumo supone un aumento de riesgo con una OR de 1,6 (IC 95%, 1,4-1,9), mientras que el consumo activo aumenta el riesgo con una OR de 2,99 (IC 95 %, 2,15-4,15), siendo mayor para la CC (OR: 5,5, IC 95 %: 3,4-8,9). El mecanismo implicado es la alteración de la barrera intestinal, la alteración de la inmunidad humoral y celular, la alteración de la microbiota intestinal y la estimulación de la fibrogénesis por estimulación del TGF-β[1],[3]. Un menor índice de masa corporal podría aumentar el riesgo de CM. No existen datos concluyentes con respecto al consumo de bebidas alcohólicas[1].
Finalmente, desde el punto de vista genético se han detectado haplotipos del complejo HLA que aumentan el riesgo para padecer una CM. Concretamente el haplotipo ancestral HLA 8.1 se asocia a la CC, aunque no a la CL. La CC también se ha asociado a alelos más frecuentes en la enfermedad de Crohn y en la colitis ulcerosa. También se ha asociado con alteraciones en el cromosoma 6 (HLA DQ2) asociado a enfermedad celíaca[1],[6].
Clinical features
The main symptom of MC is watery, chronic or intermittent, non-bloody diarrhea. The intensity of diarrhea can be variable, although the average is usually 6-7 dep/day. The onset of diarrhea may be acute in one third of cases, but it is usually insidious and before diagnosis may persist for about 6 months. Nocturnal diarrhea may be present in 25-50% of cases[2],[3].
To determine the severity of diarrhea it is recommended to use the Hjortswang criteria which state that there is clinical remission of colitis when there is an average over a week of less than 3 stools per day and less than 1 watery stool per day. There is also a CM activity index (MCDAI) that includes as severity criteria the number of unformed stools per day, nocturnal episodes, abdominal pain, weight loss, defecatory urgency and fecal incontinence. The Hjortswang criteria have been used in more studies including clinical trials, proving their usefulness in real life, so they are the ones recommended by the European guidelines[3].
The mechanism by which diarrhea occurs in MC is not completely known, but it seems to be of multifactorial origin. Firstly, there is an osmotic component since fasting improves symptoms. There is also an associated inflammatory and secretory mechanism. The role of bile acid malabsorption in the clinic of diarrhea and the pathogenesis of MC is not clearly established. Up to 44% of patients with MC have associated bile acid malabsorption demonstrated by SeHCAT. In addition, a decrease of the farnesoid X receptor at the colonic level is observed in patients with MC, and in animal studies, the use of farnesoid X receptor agonists reduces the degree of colonic inflammation. However, these are studies with limited samples[1],[2].
In addition to diarrhea, other frequent symptoms are abdominal pain (50-70 %), abdominal distention, defecatory urgency (70%) overlapping symptoms therefore with functional diarrhea or irritable bowel syndrome with predominance of diarrhea. Fecal incontinence (40%) and discrete weight loss may also occur in up to 50% of cases[2].
The presence of autoimmune diseases is more frequent in patients with MC, being present in 30-50% of cases. The most frequent of all is celiac disease, being present in 2-20% of patients with CM, recommending its serological screening in patients with CM and especially if there is no response to treatment[2],[3]. Other associated autoimmune diseases include type 1 diabetes, autoimmune thyroiditis, rheumatoid arthritis, Sjögren's syndrome and psoriasis.[2].
Natural history
CM can present as a single episode of diarrhea lasting a few months, as chronic persistent diarrhea or with intermittent episodes of diarrhea. Spontaneous remission rates are unknown, but are around 51%. In the remainder, corticosteroid dependence is observed in 22% of cases and recurrence after a first episode in 28% of cases[2],[3].
It remains unclear whether CC and CL are two histological subtypes of the same disease or are different diseases.[2]. The natural history of incomplete MC is also unknown, although data suggest that it has a greater tendency to spontaneous remission[3]. MC is not associated with increased mortality, increased risk of inflammatory bowel disease, or increased risk of colorectal cancer, so specific screening strategies for colorectal cancer are not recommended[1],[3]. Rare complications include colonic perforation spontaneously or after colonoscopy[2].
Although no increased mortality is observed, MC is associated with a lower quality of life that correlates with increased disease activity and severity of the disease and its comorbidities. Quality of life improves with budesonide treatment. However, even in the absence of activity, quality of life questionnaires provide lower scores than the healthy population, with higher prevalence of anxiety, depression and somatization[1].
Diagnosis
The diagnosis of MC, as mentioned at the beginning, is based on the finding of defined histological features in colonic biopsies obtained by colonoscopy. Therefore, the performance of colonoscopy, the taking of biopsies and their subsequent anatomopathological analysis are crucial for the diagnosis. This is due to the fact that neither from the clinical nor analytical point of view, nor from the macroscopic findings of colonoscopy, are there criteria to establish a diagnosis.
The differential diagnosis of chronic watery diarrhea includes organic processes such as infections, celiac disease, inflammatory bowel disease, bacterial overgrowth and colon cancer. However, functional pathology such as diarrhea-predominant irritable bowel syndrome and chronic functional diarrhea are also included[8]. In a meta-analysis it was observed that 33.4% of cases with CM would meet the diagnostic criteria for IBS-D. In another study, between 6-9% of cases with CM met the diagnostic criteria for IBS-D. In another study, 6-9% of patients with IBS-D and chronic functional diarrhea actually had MC when colonoscopy with biopsies was performed[1],[3]. In an attempt to reduce the number of colonoscopies and biopsies and increase the diagnosis of MC, a scoring system was established. This system scores age greater than or equal to 55 years, diarrhea course of less than or equal to 6 months, 5 or more bowel movements per day, body mass index less than 30 kg/m2, active smoking, and treatment with NSAIDs or SSRIs. A score greater than or equal to 10 had a sensitivity of 91-93 % with a specificity of 49 % for the diagnosis of MC (Table 2)[9] However, the recommendations of the European and Spanish MC guidelines state that colonoscopy with biopsies should be performed in patients with a clinical diagnosis of IBS-D or functional diarrhea, when there is no response to treatment or when there are risk factors for MC. The recommendations of the AGA regarding the performance of colonoscopy with biopsy in the context of IBS-D and functional diarrhea are more ambiguous, considering them as not necessary in the absence of alarm symptoms or in children under 50 years of age in cases of IBS-D, although it refers that it is the only method to rule it out in cases of FD[8].
Table 2
Predictors of CM in chronic diarrhea. BMI: Body mass index. SSRIs: Selective serotonin reuptake inhibitors. SNRI: Serotonin-norepinephrine reuptake inhibitors. NSAIDs: Non-steroidal anti-inflammatory drugs.
| Predictors of CM in chronic diarrhea[9]. | |
| Factor | Points assigned |
| Age ≥ 55 years | 6 |
| Duration of diarrhea ≤ 6 months. | 5 |
| BMI less than 30 kg/m2 | 3 |
| Number of bowel movements ≥ 5 /d (mean since symptom onset) | 3 |
| Active smoking | 3 |
| Current treatment with SSRIs or SNRIs | 2 |
| Current treatment with NSAIDs | 2 |
| Score ≥ 10 points: sensitivity 91-93 %, specificity 49 % for the diagnosis of CM. | |
Laboratory tests are useful in the differential diagnosis with other organic disorders, such as, for example, stool stool cultures or parasites to rule out infectious processes or serology for celiac disease. Celiac disease is frequently associated with CM and should be ruled out[3]. Regarding fecal biomarkers, there are no studies to support their use for the diagnosis or follow-up of CM. Although fecal calprotectin in some studies shows discretely elevated levels in MC versus functional disorders, its predictive value is very low and the European guideline discourages its use[3].
Colonoscopy with ileoscopy is indicated in the study of chronic diarrhea[2],[3]. Macroscopic findings of the colonic mucosa in MC are generally normal when colonoscopy is performed. However, nonspecific findings such as edema, erythema, nodularity, altered vascular patterns, linear erosions and pseudomembranes may be found in up to 40% of cases. No differences in these findings have been demonstrated between LC and CC[3].
In the context of chronic watery diarrhea with normal macroscopic findings, colonic biopsies are considered essential, because MC is the most frequent cause of chronic diarrhea with normal endoscopic findings[2]. In addition, it can also diagnose some cases of Crohn's colitis or infectious colitis. Biopsy collection is cost effective in the context of chronic watery diarrhea and its ratio is superior to duodenal biopsy collection in the study of diarrhea, anemia or first-degree history of celiac disease[2]. Biopsy collection should be performed perpendicular to the colon wall, to facilitate the measurement of the collagenous band in the case of CC diagnosis. There is consensus that biopsies should be taken in separate canisters from the right and left colon. Although the clinical usefulness of separating these canisters is controversial, it can help the diagnosis given the difference in cellularity in the lamina propria of the right and left colon. According to the Spanish clinical guidelines, at least 2 biopsies should be taken from the ascending, transverse, descending and sigmoid colon[2]. The European guidelines recommend taking biopsies from the right and left colon, without specifying the specific location or number of biopsies[3]. In all cases of MC it is recommended to rule out the coexistence of celiac disease. However, the study of bile acid malabsorption is not recommended[3].
Histological diagnosis
From the definition of MC derives the importance of a careful histological study of the submitted specimens, always taking into account the histological characteristics of the colon in each of its locations. The specification of the location is essential to avoid misinterpretation.
The histological criteria for microscopic colitis have been established with a certain rigidity, a fact that leads to the suspicion that it is not easy to differentiate two pictures with similar findings, while at the same time it is deduced that these criteria could change depending on the establishment of a consensus that is more rigid or flexible and to which it is necessary to adapt.
The criteria are the following:
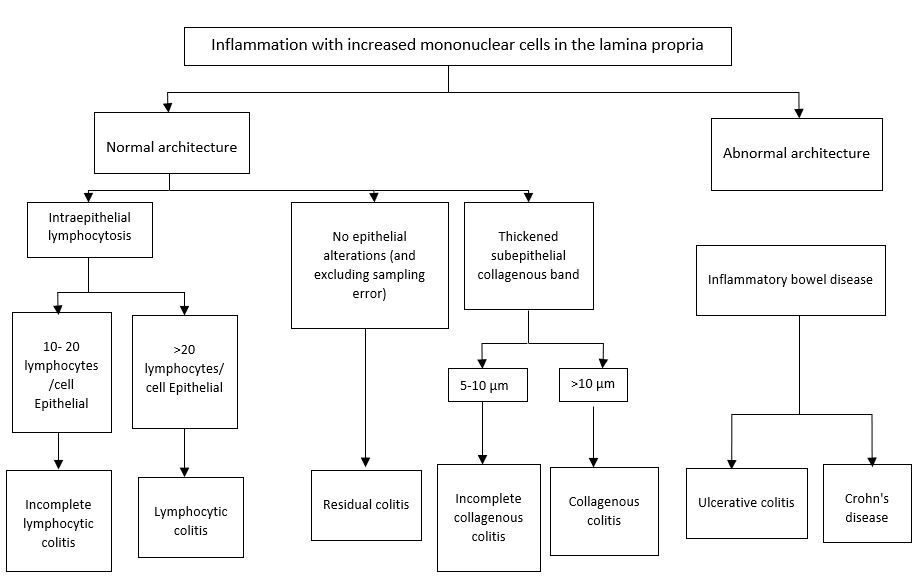
Lymphocytic colitis
• Intraepithelial lymphocytosis (20 intraepithelial lymphocytes / 100 epithelial cells) without associated architectural distortion of the crypts. This counting can, if necessary, be supported by the use of immunohistochemical techniques that reveal the presence of T lymphocytes in the sample. The CD3 marker is generally used for this purpose, and it should be noted that the samples evaluated with this stain end up obtaining slightly higher T lymphocyte counts than those obtained with routine stains (hematoxylin and eosin, HE).
• Perinuclear lymphocytic halo (not always present).
• Degenerative or regenerative changes of the superficial epithelium, variable (flattening, vacuolization, mucin depletion...).
• Only discrete thickening of the subepithelial collagenous band (less than 10 μm).
• Increased cellularity in the lamina propria, with frequent presence of eosinophils.
• Neutrophilic cryptitis and cryptic abscesses may be present but neutrophilic activity may only be focal[10],[11].
Collagenous colitis
• Thickening of the subepithelial collagen band at the superficial level (greater than 10 μm).
• The thickening is easier to identify between the crypts.
• Within the band we can find capillaries, red blood cells and inflammatory cells.
• Increased epithelial damage and, therefore, more frequent detachment of the surface epithelium.
• An increase in the number of intraepithelial lymphocytes can be identified, which is minor and not necessary for diagnosis.
• Histochemical techniques can be used to demonstrate the collagen band (Masson, tenascin...).
• Similar criteria at the lamina propria level as LC[10],[11].
Incomplete MC
• The clinical features are consistent with the entity, but the characteristic histology is incomplete (the minimum number of intraepithelial lymphocytes or the minimum thickness of the stratum collagen is not reached).
• Increased number of intraepithelial lymphocytes but less than 20/100.
• Increased subepithelial collagenous layer thickness but less than 10 μm[12].
Treatment
Treatment with oral budesonide is the treatment of choice to achieve remission in MC (Figure 3). It is a treatment approved by the European Medicines Agency, and although neither this nor any other is approved by the FDA, it is recommended by the American, Spanish and European MC guidelines[1],[3]. With moderate evidence in CC and low evidence in LC, treatment with budesonide achieves a histological clinical response and an improvement in quality of life[3].
Figure 3
Treatment scheme for active MC. Induction budesonide: 9 mg/24h/voral for 6-8 weeks. Maintenance: 3-6 mg/24h/voral. Cholestyramine: 3-4 gr/8-12h/voral. Loperamide: 2-16 mg/24h/voral.
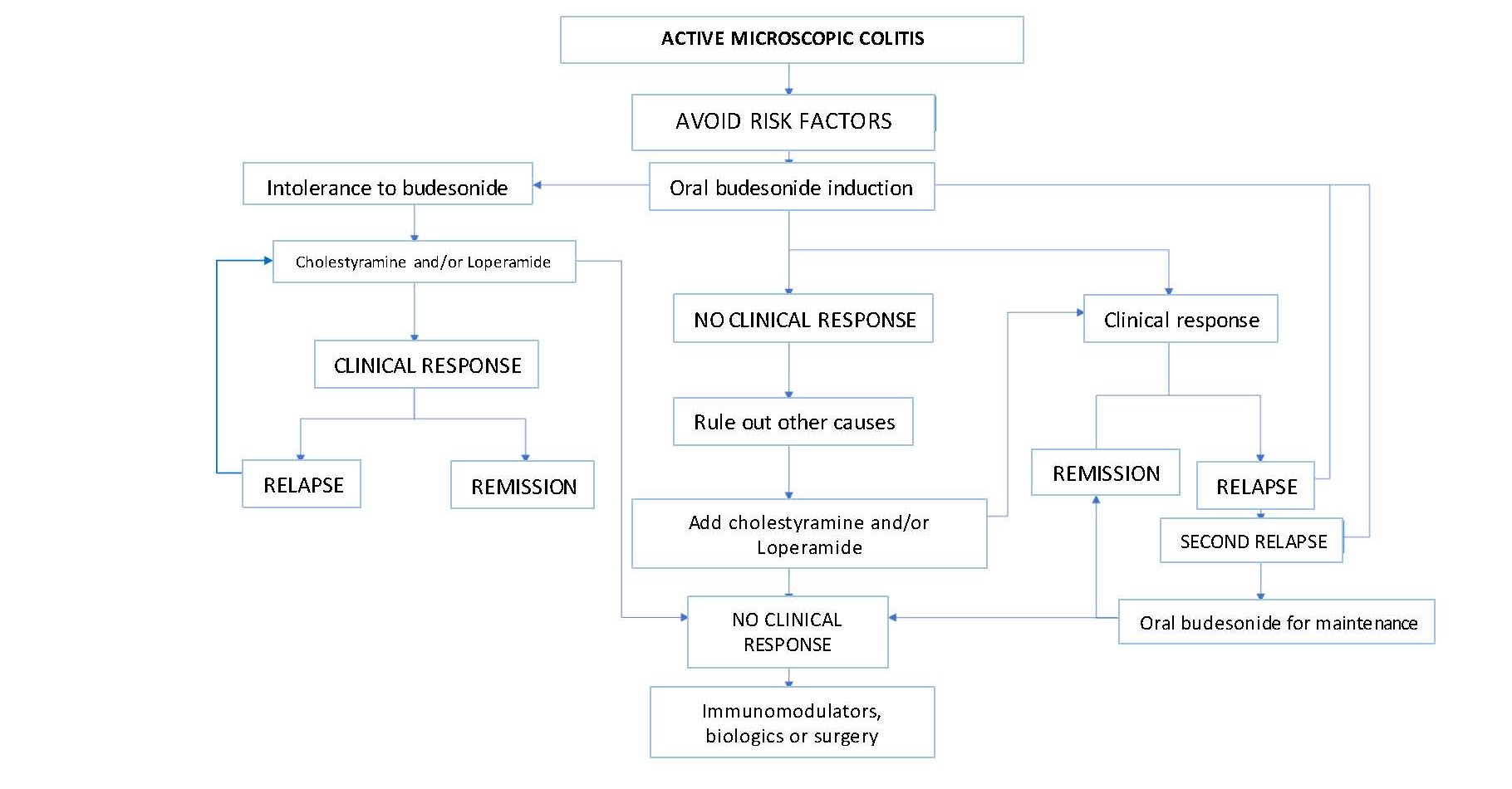
Treatment with oral budesonide is the treatment of choice to achieve remission in MC (Figure 3). It is a treatment approved by the European Medicines Agency, and although neither this nor any other is approved by the FDA, it is recommended by the American, Spanish and European MC guidelines[1],[3]. With moderate evidence in CC and low evidence in LC, treatment with budesonide achieves a histological clinical response and an improvement in quality of life[3].
Induction treatment is at a dose of 9 mg/day orally for 6-8 weeks, with a remission rate of 81% in CC and 95% in LC. Neither progressive dose reduction nor concomitant use of calcium and vitamin D is necessary[3],[13],[14]. Nor is it necessary to confirm histologic response by repeat colonoscopy with biopsies[3].
Despite achieving high induction rates, recurrence is frequent. Therefore, when a second relapse occurs after induction treatment, maintenance treatment with budesonide is recommended, with greater evidence in CHD. The doses used in the research studies were 6 mg/day, or alternating 3 and 6 mg each day, with the recommendations of the European guidelines being to try to use the lowest effective dose[2],[3]. Long-term use of budesonide is safe. Although there could be a decrease in bone mineral density with maintenance treatment, no increase in the risk of fractures has been demonstrated, so although some authors recommend adding vitamin D and calcium, especially if other risk factors for osteoporosis coexist, the European guidelines do not[3],[13].
In cases in which there is no response to induction treatment with budesonide, it is recommended to rule out other causes of chronic diarrhea, such as bile acid malabsorption, irritable bowel syndrome or celiac disease. In addition, discontinuation of smoking and of drugs related to MC is recommended, although the evidence for these measures is scarce and is usually considered at the time of diagnosis of the disease. Once these premises have been met, if symptoms persist, the first recommended measure is to add cholestyramine and/or loperamide to the treatment. Both drugs can also be used in mild cases of the disease (less than 3 dep/day, and less than 1 watery stool per day)[3],[13],
Cholestyramine (3-4 gr/ 2 or 3 times a day) has shown efficacy in remission, especially when there is an association of MC with bile acid malabsorption. In this sense, the European guidelines recommend its use, with low evidence, only in cases in which both diseases coexist, while the Spanish guidelines do not make such differentiation[2],[3].
Loperamide (2-16 mg/day) has no controlled studies that support its efficacy in MC. Based on case series, it is recommended to reduce the number of bowel movements, improve fecal incontinence and therefore quality of life. No effect on the pathogenesis of the disease is attributed to it and it is considered a symptomatic treatment[2],[3].
The use of antibiotics, probiotics, mesalazine, bismuth subsalicylate or other corticosteroids in the treatment of the disease is not recommended[1]-[3]. When there is no response to induction treatment with budesonide or budesonide plus cholestyramine/loperamide, or to maintenance treatment with budesonide, CM is considered refractory. In these cases, the recommendations are the use of immunomodulators such as azathioprine or 6-mercaptopurine, and among biologics, anti-tumor necrosis factor drugs and vedolizumab. The use of methotrexate is not recommended. However, experience is scarce and cases should be selected[3].
Finally, surgery (ileostomy, sigmoidostomy, or proctocolectomy with ileoanal pouch) could be a rescue treatment in very selected cases[3].
Conclusion
>MC is a disease of increasing incidence and prevalence. Although it is not associated with increased mortality, it has a negative impact on the quality of life of patients. Its pathogenesis is unknown and progress must be made in this regard to improve the understanding of the disease and finally establish the relationship between lymphocytic and collagenous colitis and its natural history. Diagnosis still depends on colonoscopy with colonic biopsies. One line of research would be to search for biomarkers of the disease or to develop new clinical scoring studies to predict the risk of MC. This would avoid performing colonoscopies and taking biopsies in patients with functional pathology. Taking biopsies in separate left and right colon bins is recommended; although this circumstance, along with the number of biopsies required, should be clarified in the future. In addition, the natural history and clinical relevance of incomplete MC should be determined. Budesonide is the treatment of choice with frequent need for maintenance treatment with this drug, which has a good safety profile. New drug studies would be necessary in case of refractoriness to budesonide.