
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Díaz Brito JA, Herrera Gutiérrez L, Grilo Bensusan I. Transanal extraction of a giant calcified fecaloma. RAPD 2025;48(2):80-81. DOI: 10.37352/2025483.5
Introduction
Chronic constipation can sometimes cause the formation of hard stools in the rectum or colon, which cannot be expelled spontaneously and are known as fecalomas. There are few published cases of calcified giant fecalomas and the method of removal used has not been previously described in the literature.
Clinical case
We present the case of a 75-year-old woman who came to the surgery consultation because of pain in the hypogastrium of more than one year of evolution. In addition, she presented liquid diarrhea without pathological products accompanied by rectal tenesmus and sensation of incomplete evacuation. No rectal or abdominal masses were palpable.
She had been previously referred to Gynecology by her primary care physician due to the finding of a calcification in the pelvic area observed in an abdominal X-ray, ruling out pathology in this area (Figure 1A).
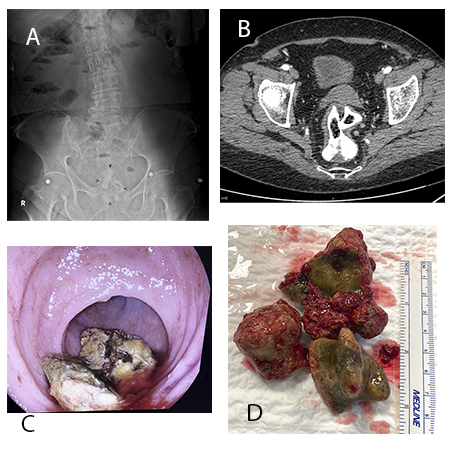
Figure 1
A: Abdominal X-ray showing a calcified lesion in the rectum (arrowheads). B: Abdominal CT scan of the pelvis showing the calcified fecaloma in the rectum. C: Colonoscopy image with calcified fragments of the fecaloma after the rupture procedures. D: Stone fragments of the extracted fecaloma.
An abdominopelvic CT scan with contrast was indicated, showing the existence of a rectal occupation by a densely calcified material measuring 7 x 9 cm, with digitiform extensions suggestive of calcified fecaloma (Figure 1B).
A colonoscopy confirmed the existence of a stony fecaloma at the rectal level that could not be passed, nor could it be approached for fragmentation due to its size, consistency and shape. Given the impossibility of endoscopic treatment, nor response to treatment with enemas, it was decided to extract the fecaloma transanal with surgical instruments. For this purpose, under general anesthesia and in lithotomy position, the fecaloma was fragmented and several fragments were extracted using Rochester forceps with teeth, Foester forceps and hemostasis forceps. Intraoperative colonoscopy was performed and other fragments were extracted by means of a polypectomy loop, leaving the entire rectum and rectosigma free (Figures 1C and 1D). Postoperative evolution was satisfactory, tolerating oral diet at 24 hours, presenting normal stools at 48 hours and being discharged at 72 hours.
Discussion
The usual treatment of fecalomas is conservative with the use of enemas and digital extraction.[1]. E Endoscopic treatment by injection with sclerosis needles of different substances and their fragmentation and extraction with a polypectomy loop or biopsy forceps represents a new therapeutic step.[2]. If the previous measures fail, surgical removal by laparotomy can be considered, sometimes associating partial colectomies. [3]. This case is interesting because of the exceptional nature of calcified fecalomas and the success of a technique, whose previous description we have not found in the medical literature and which could be an option to avoid laparotomy[4],[5].