
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Giráldez Jiménez MD. High-risk Gastrointestinal Cancer Clinic. RAPD 2025;48(3):105-111. DOI: 10.37352/2025483.3
Introduction
Approximately 5-10% of cancers are hereditary, i.e., they are due to germline mutations in certain genes[1].Patients carrying these mutations are at high risk of developing cancer. There are also familial forms of cancer in which we observe an aggregation of cases in the family, but no genetic alteration responsible is identified.
Colorectal cancer is one of the cancers with the highest frequency of hereditary and familial forms, so it is essential to identify individuals at increased risk to establish appropriate preventive programs[2].In this sense, the High-Risk Colorectal Cancer Clinics emerged in the Gastroenterology Units to offer specific and specialized care to the population at high risk of colorectal cancer[3]. In recent decades, the spectrum of these clinics has been expanding to cover other digestive neoplasms, so that we can now call them High-Risk Gastrointestinal Cancer Clinics or Gastrointestinal Cancer Prevention Clinics. Two main factors have determined this evolution: 1) The implementation of multigene panels for genetic analysis, which allows us to diagnose a greater diversity of hereditary cancer syndromes[4]-[8]; and 2) The growing evidence of the effectiveness of screening in individuals at high risk of digestive neoplasms other than colorectal cancer such as, for example, pancreatic cancer[9]-[12].
High-Risk Gastrointestinal Cancer Clinics vs. Genetic Counseling Units
In parallel to the development of High-Risk Gastrointestinal Cancer Clinics, many centers have established Genetic Counseling Units. Although both models are aimed at the care of the population at high risk of cancer, they present important differences in their structure. High-Risk Gastrointestinal Cancer Clinics are coordinated by gastroenterologists with training in Genetics, focus on the prevention of digestive neoplasms, and offer coverage to both familial and hereditary forms of these neoplasms. In contrast, Genetic Counseling Units are coordinated by geneticists or, more frequently, oncologists and cover all types of hereditary neoplasms. Furthermore, while the objective of the HHigh-Risk Gastrointestinal Cancer Clinic is the comprehensive care of such individuals, including diagnosis, follow-up, and treatment if necessary, many Genetic Counseling Units focus their activity mainly on diagnosis and refer individuals to the relevant specialists after diagnosis. Therefore, these are two different models that can coexist without problem in tertiary centers to ensure comprehensive care for all types of hereditary cancer syndromes.
Fundamental characteristics of High-Risk Gastrointestinal Cancer Clinics
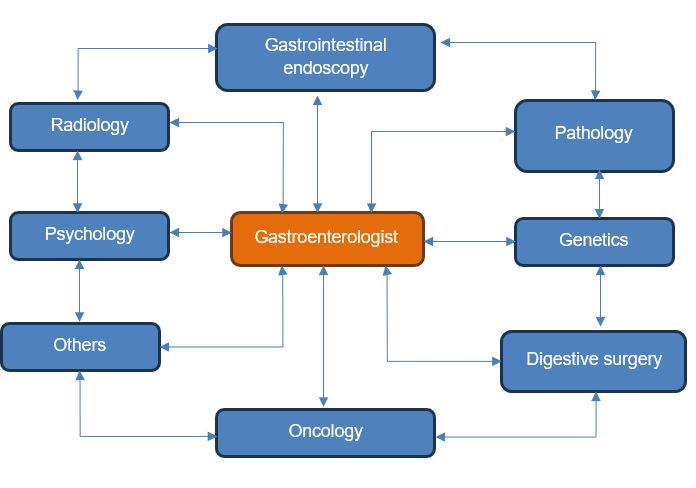
As previously mentioned, High-Risk Gastrointestinal Cancer Clinics are led by gastroenterologists who must be trained in Genetics. However, to meet the objective of providing comprehensive care to individuals at high risk of digestive neoplasms, the participation of a multidisciplinary team is essential for the different stages of diagnosis, follow-up, and treatment (Figure 1). In this regard, the role of specialties such as Pathology (including molecular pathology studies), Genetics (with the capacity to perform new generation sequencing), Radiology (including advanced imaging techniques), Digestive Endoscopy (including advanced endoscopic techniques, both diagnostic and therapeutic), Digestive Surgery, Oncology, Gynecology, Clinical Psychology, and many others that may vary depending on the type of syndrome identified (for example Urology, Dermatology, etc.) should be highlighted.
Figure 1
Multidisciplinary team of the High-Risk Gastrointestinal Cancer Clinics. The High-Risk Gastrointestinal Cancer Clinics is coordinated by a gastroenterologist with expertise in Genetics but requires the participation of a multidisciplinary team to ensure comprehensive care for high-risk patients.
High-Risk Gastrointestinal Cancer Clinics have distinct characteristics that set them apart from other Digestive System Consultations. In these specialized clinics, while we do care for patients, we often focus on healthy individuals as well. Additionally, the emphasis in these clinics is on the family unit rather than the individual patient, which is typical in other healthcare settings. The main objective of the High-Risk Gastrointestinal Cancer Clinic is prevention and early diagnosis, whereas other consultations generally focus the treatment of existing digestive disorders.
Criteria for referral to the High-Risk Gastrointestinal Cancer Clinic
All patients with suspected hereditary or familial digestive cancer should be referred for evaluation in a High-Risk Gastrointestinal Cancer Clinics. In general, this suspicion is established by the occurrence of multiple tumors in a patient or a family, by the diagnosis of neoplasms at early ages or by rare tumors.
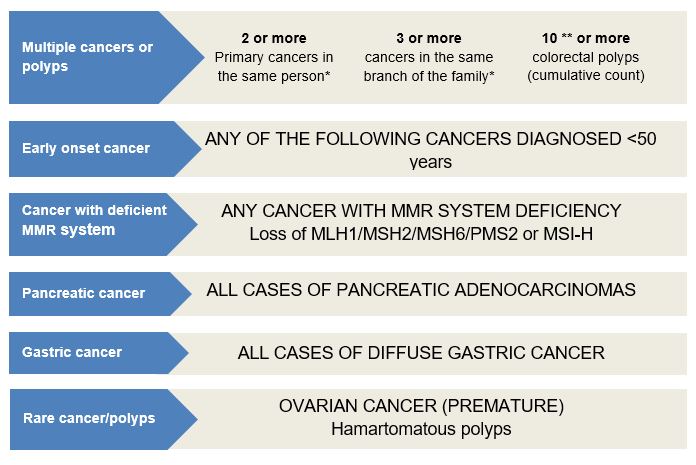
As a guideline, we could suggest more specific referral criteria as outlined in Figure 2. It should be noted that in those centers with a Genetic Counseling Unit, some of these patients may be initially seen. However, we believe that in those cases where a syndrome is suspected, in which the most frequent manifestation is the development of a digestive tumor (for example, Lynch syndrome), referral to a High-Risk Gastrointestinal Cancer Clinic would be more appropriate to ensure comprehensive care.
Figure 2
Criteria for referral to the High-Risk Gastrointestinal Cancer Clinics * Mainly digestive tumors or Lynch-spectrum neoplasms (stomach, endometrium, ovary, urothelial tumors, biliary tract and brain) ** In the case of adenomatous polyps. For serrated polyps the criteria for referral would be: Criteria 1) ≥ 5 serrated polyps proximal to rectum, all size ≥ 5 mm, with 2 being ≥ 10 mm ; or Criteria 2) > 20 serrated polyps of any size along the large bowel, ≥ 5 proximal to the rectum. MMR system = DNA mismatch repair system.
Schedule of visits in the High-Risk Gastrointestinal Cancer Clinic
Patient management in the High-Risk Gastrointestinal Cancer Clinic is organized according to the following schedule of visits:
First visit: Cancer genetic risk assessment. Genetic counseling 1 (pre-test).
Second visit: Genetic counseling 2 (post-test). Establishment of a personalized preventive program.
Third and subsequent visits. Follow-up visits.
First visit
The main objective of this visit is to assess the genetic risk of cancer in the family. For this purpose, our main tool is the family history or pedigree. In this first visit, we will draw a detailed family tree that encompassess at least three generations, including all cases of both benign and malignant neoplasms (type, location, and age at diagnosis), as well as the age and cause of all deaths. To draw a family tree with high-quality information, it is important that the patients are notified before the visit, so that they can review the necessary information and, if possible, provide reports of the cases of neoplasia. Likewise, on our part, it is essential to verify as far as possible all the information provided by checking the electronic medical records available to us. It should be emphasized that, although building a family tree is laborious and time-consuming, it should not be replaced by a written collection of family history in the medical record. In this sense, the pedigree is much more useful since it provides a visual snapshot of the family, in which we identify cancer cases but also the family structure, detect if the family is not very informative (small size, numerous cases of death at early ages due to causes other than cancer, little information available on any family branch, etc.), visualize possible inheritance patterns and identify all the individuals at risk that we would have to evaluate in the case of establishing the diagnosis of a hereditary syndrome.
In addition to the family tree, there are other tools that help us to establish the genetic risk of cancer. In this sense, the pathology reports of the tumors diagnosed in the family are of great help. Sometimes, we also have tumor molecular studies that allow us to assess the status of the DNA mismatch repair system (MMR system), such as immunohistochemistry of MMR system proteins and microsatellite instability. These molecular tests are performed as screening for Lynch syndrome, as this syndrome is caused by a mutation in a gen of the MMR system and is characterized by a malfunction in this system, resulting in the appearance of microsatellite instability and/or loss of expression of the protein corresponding to the mutated gene[13]. According to current guidelines, all patients diagnosed with colorectal cancer should undergo molecular screening for Lynch syndrome[14]-[16].
Gastrointestinal endoscopy reports can also be useful, especially colonoscopy reports in cases of polyposis (characteristics, location, and number of polyps).
Predictive models have been developed that, based on personal and family history, allow us to establish the probability of an individual carrying a mutation in the genes of the MMR system (for example, the PREMM5 model)[17] or in a broader panel of genes (PREMMplus model)[18].
Finally, the tool that will allow us to confirm the diagnosis of a suspected hereditary syndrome is germline genetic testing (performed in blood or saliva). Classically, a single gene or a small number of genes were studied using Sanger sequencing. In recent decades, thanks to the development of next-generation sequencing (NGS) technologies, it has become increasingly common to perform multigene panels (including in the panel genes associated with colorectal cancer, digestive neoplasms, or cancer in general) or even to sequence the entire exome (coding part of the DNA).
During this initial visit, if we identify any suspicion of a hereditary syndrome within the family and a germline genetic study is recommended, we will conduct pre-test genetic counseling before proceeding with the request (refer to the section on Genetic Counseling).
Second
In this visit, we have already received the requested results of the genetic study, and we will carry out a post-test genetic counseling to inform the patient (see section on Genetic Counseling). We will plan a personalized preventive program based on their genetic testing results, which may include endoscopic and/or radiological surveillance, preventive surgeries, and, in some cases, chemopreventive strategies. Likewise, if a pathogenic variant is identified in any of the evaluated genes, we will initiate cascade genetic screening in first-degree relatives. Finally, the identification of a germline mutation can be useful if the patient requires oncological treatment since it allows us to choose genotype-based treatment.
Third and subsequent visits
Since the objective of the High-Risk Gastrointestinal Cancer Clinic is providing comprehensive care of high-risk individuals, patients will not be discharged after a diagnosis of a hereditary syndrome, instead, we will follow them with a periodicity determined by the preventive program that we establish and surveillance findings.
Indications for multigene panel testing
At present, both the indications for multigene panel testing and the genes that should be included in such studies are subject to debate. Different societies have published recommendations in this regard with the aim of unifying criteria and trying to make the studies cost-effective. However, given that the main limiting factor is economic, it is foreseeable that as prices continue to decrease, the indications for multigene panel testing will expand. Some guidelines that can serve as a reference for clinical practice in the consultation of High-Risk Gastrointestinal Cancer Clinics are those published by the following societies:
Collaborative Group of the Americas on Hereditary Gastrointestinal Cancer[19] (recommendations only for colorectal and/or polyposis cancer)
American Society of Clinical Oncology (ASCO)[20]
National Comprehensive Cancer Network (NCCN):
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1544 (colorectal, endometrial, and stomach cancer).
https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1545 (pancreas, breast, ovarian and prostate).
Joint position document of the Spanish Association of Gastroenterology (AEG), Spanish Society of Medical Oncology (SEOM), Spanish Association of Human Genetics (AEGH) and IMPaCT-GENÓMICA consortium[21].
Interpreting genetic test results
When a genetic study identifies genetic variants in any of the evaluated genes, these should be classified according to the recommendations of the American College of Medical Genetics (ACMG) in one of the following categories[22]:
Benign variant
Likely benign variant
Variant of uncertain significance
Likely pathogenic variant
Pathogenic variant
In practice, both benign and likely benign variants are considered as a single category. These variants do not affect the function of the corresponding protein and therefore, from a clinical point of view, do not require any action. Likewise, pathogenic and likely pathogenic variants are considered as a single category. These variants allow us to diagnose a hereditary syndrome and their identification has clinical implications. In those cases in which we have performed multigene panel testing or whole exome sequencing, we may encounter different clinical scenarios. The ideal scenario would be to identify a pathogenic variant in a high penetrance gene that fits well with the phenotype of the family, since in these cases the diagnosis is solid and we will have well-established clinical guidelines for the follow-up of carrier individuals. A second scenario would be to identify a pathogenic variant in a gene with high penetrance but that does not match well with the family phenotype (e.g., amutation in the BRCA2 gene in a family that meets the Amsterdam criteria). In these cases, we cannot establish that the family phenotype is secondary to the identified variant and in addition to the preventive measures recommended in the clinical guidelines for the diagnosed syndrome, we should consider additional preventive measures based on the family phenotype (in our example, consider colorectal cancer screening in carriers). Finally, we may find a pathogenic variant in a gene of moderate penetrance. In these cases, we will not have well-established clinical practice guidelines to guide us since the available evidence is usually quite limited and recommendations change frequently as new studies are published
Finally, in cases where variants of uncertain significance are identified, we will not have sufficient evidence to propose a preventive program focused on the risks associated with the corresponding gene alteration. In this situation, we should periodically review the variant in the available databases as it may end up being reclassified as benign or pathogenic, which will allow us to modify our recommendations accordingly in individuals who are carriers[23],[24].
Genetic counseling
Genetic counseling was legally regulated in Spain in 2007 by the Biomedical Research Law (Law 14/2007 of July 3). This law defines genetic counseling as the "procedure aimed at informing a person about the possible consequences for him or her or his or her offspring of the results of a genetic analysis or screening and its advantages and risks and, where appropriate, to advise him or her about the possible alternatives derived from the analysis. It takes place both before and after a genetic test or screening and even in the absence of the same".
In addition, some Autonomous Communities also have laws that regulate genetic counseling, such as the Order of March 3, 2005, of the Regional Ministry of Health, which regulates the organizational devices that carry out genetic counseling in cancer in the Valencian Community, or Law 11/2007, of November 26, 2007, regulating genetic counseling, the protection of the rights of persons who undergo genetic analysis and human DNA banks in Andalusia.
Genetic counseling must be carried out in two phases, one before requesting the test (pretest genetic counseling) and the other after receiving the test results (posttest genetic counseling).
Pre-test genetic counseling
Pre-test genetic counseling is essential for the patient to understand the implications of undergoing a genetic study and to be able to make informed decisions about accepting or declining genetic testing. It is key for the patient to understand the overall benefits, risks, and limitations of the study, as adequate information at this stage can facilitate adaptation to the results later on. Some key points to address during this phase of genetic counseling are as follows:
Provide general information about the test and its purpose.
Description of the disorder(s) included in the test.
Advantages, risks, and limitations of the test.
Confidentiality of the information obtained in the test and the need for authorization prior to its performance (informed consent).
Explanation of the possible results: positive, negative, variants of uncertain significance, and secondary or unexpected results.
How these results would be interpreted according to the patient's family and medical history.
Possible medical, reproductive, and psychosocial implications of genetic test results, including implications for family members.
Management options without genetic test results compared with recommendations associated with possible test results.
Patient education and support.
Regarding the benefits of genetic testing, it is important to convey to the patient that if the diagnosis of a hereditary syndrome is established, it will be possible to design an individualized surveillance strategy according to his or her specific cancer risk. Furthermore, depending on the syndrome, surgical options can be considered to reduce the risk of cancer development. On the other hand, if the patient develops cancer, we will be able to adapt the treatment recommendations according to the results of the genetic tests. Finally, we will be able to study family members at risk and offer specific preventive measures to those who are carriers.
On the other hand, it is important to emphasize that the test does not always allow us to reach a diagnosis and that we may obtain results that are difficult to interpret (for example, variants of uncertain significance) or unexpected (incidental findings, i.e., that are not related to the reason for which the test was requested and that may or may not have implications for health and clinical significance)[25].
Post-test genetic counseling
This second phase of genetic counseling focused on clearly explaining the results obtained from the test and their implications. When diagnosing a hereditary syndrome, we will estimate the associated cancer risks and establish an appropriate prevention plan. We will also ask the patient to share genetic testing results with first degree relatives to set up a cascade genetic screening.
We should also bear in mind that the results of the genetic study may have implications for the choice of oncological treatments if the carrier is a patient with cancer or develops cancer during follow-up.
Conclusions
The High-Risk Gastrointestinal Cancer Clinic provides comprehensive care (identification, follow-up, and treatment if necessary) and specialized care for individuals at high risk of developing colorectal cancer and/or different digestive neoplasms. This model of care is currently very useful because the increasing implementation of next-generation sequencing in clinical practice (multigene panel testing and even whole exome sequencing) has resulted in the identification not only of a greater proportion of hereditary colorectal cancer syndromes,but also of a broader variety of hereditary syndromes, some of which confer a high risk of certain digestive neoplasms that can benefit from appropriate preventive programs. To set up a High-Risk Gastrointestinal Cancer Clinic, it is necessary to have gastroenterologists with training in Genetics and a multidisciplinary team that includes, among others, specialties such as Genetics, Pathology, Radiology, Digestive Endoscopy, Digestive Surgery, Oncology and Clinical Psychology. This approach emphasizes the family rather than just the individual patient, aiming primarily to prevent the development of digestive neoplasms in those recognized as being at high risk, as well as in all family members who share this increased risk.