
 Descargar número completo
Descargar número completo Download full issue
Download full issueCORRESPONDENCE
Ana Torres Domínguez
Costa del Sol University Hospital. Marbella, Málaga.
29603 Marbella, Málaga
CITATION
Torres Domínguez A, Jofré Peralta S, Rivera Irigoin R. Gastrostomy tube dislodgement into the peritoneal cavity after its manual insertion. RAPD 2024;47(1):43-44. DOI: 10.37352/2024471.6
Introduction
Percutaneous endoscopic gastrostomy is a technique that involves the placement of a tube through the abdominal wall using different techniques for the administration of fluids, enteral nutrition and/or medication or for gastric decompression. The most frequent related complications are peristomal leakage and infection, tube obstruction or tube dislodgement, among others[1],[2]. Accidental removal of the gastrostomy tube is one of the most frequent reasons for consultation of these patients in the emergency department, and is resolved in most cases after manual insertion of a new tube.
Clinical case
An 84-year-old woman with no known previous personal history was diagnosed with oropharyngeal neoplasia. Due to dysphagia and inability to meet her nutritional requirements, a percutaneous gastrostomy was performed endoscopically for enteral nutrition by means of a direct introduction technique through gastric pexias. The procedure passed without complications and enteral nutrition could be started without incident.
Five weeks later, she came to the emergency department due to accidental removal of the feeding tube at home, and a new one was inserted blindly by hand through the previous stoma, with no immediate complications.
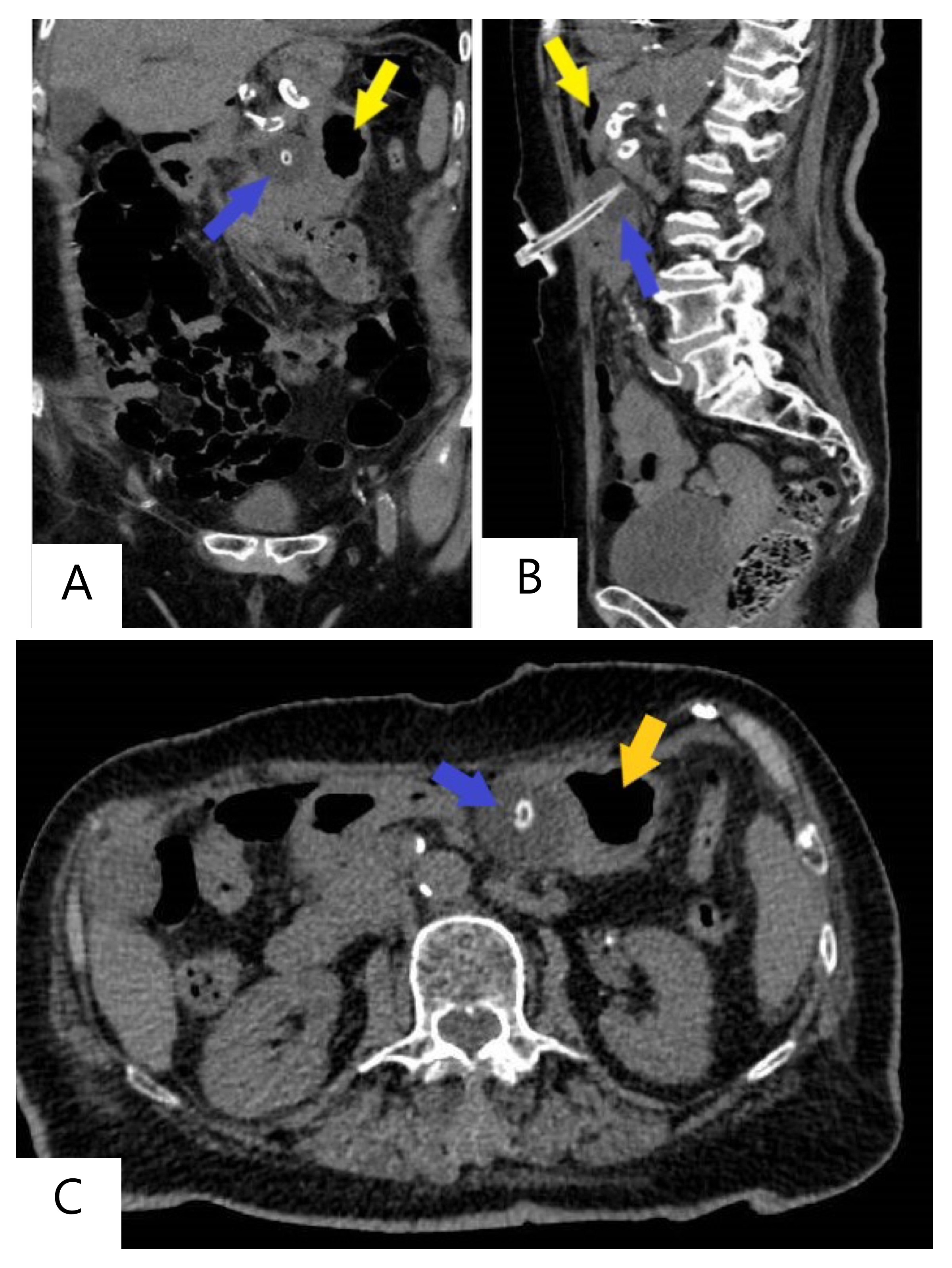
Twenty-four hours later, she was seen again for severe abdominal pain after administration of enteral nutrition through the tube, with no fever or other associated symptoms. An urgent computed tomography (CT) scan was performed, which revealed a dislodgement of the tube, identifying the distal end in the peritoneal cavity, outside the gastric cavity (Figure 1). The tube was removed and empirical antibiotic therapy with metronidazole was started, and a new percutaneous endoscopic gastrostomy was performed. The patient progressed favourably until the condition was resolved.
Discussion
Dislodgement of the gastrostomy tube is a complication that can occur after tube removal (accidental or due to tube defect) in patients with an immature gastrocutaneous fistula (less than 4 weeks old) in which the stomach serosa has not properly adhered to the parietal peritoneum, and manual blind reinsertion in these patients should be avoided[1],[3].
Although manual insertion is considered safe after 4 weeks, as in this case, it is important to detect this complication early, and in case of doubt, a water-soluble contrast study should be performed to confirm the correct placement of the tube before feeding is started[3].