
 Descargar número completo
Descargar número completo Download full issue
Download full issueCite this work
Vergara Ramos J, Abraldes Bechiarelli AJ, Rodríguez Amado MA, Pérez Monzú A, Rodríguez Ramos C. Disimpaction of fecaloma with Coca-Cola® injection. RAPD 2025;48(4):138-140. DOI: 10.37352/2025484.3
Introduction
Fecal impactions are caused by a mass of hard stool that accumulates mainly in the distal colon and rectum. Factors that can contribute to their formation include chronic constipation, anorectal anatomical abnormalities, advanced age, and certain neuropsychiatric disorders. Management is usually conservative, involving oral laxatives, enemas, and sometimes even digital disimpaction. Complications are rare, but when they do occur, they may require surgical intervention[1].
Below, we present a case of a fecal impaction that did not resolve with conservative treatment and was successfully treated by endoscopic fragmentation with the help of Coca-Cola®, avoiding surgery for the patient.
Clinical case
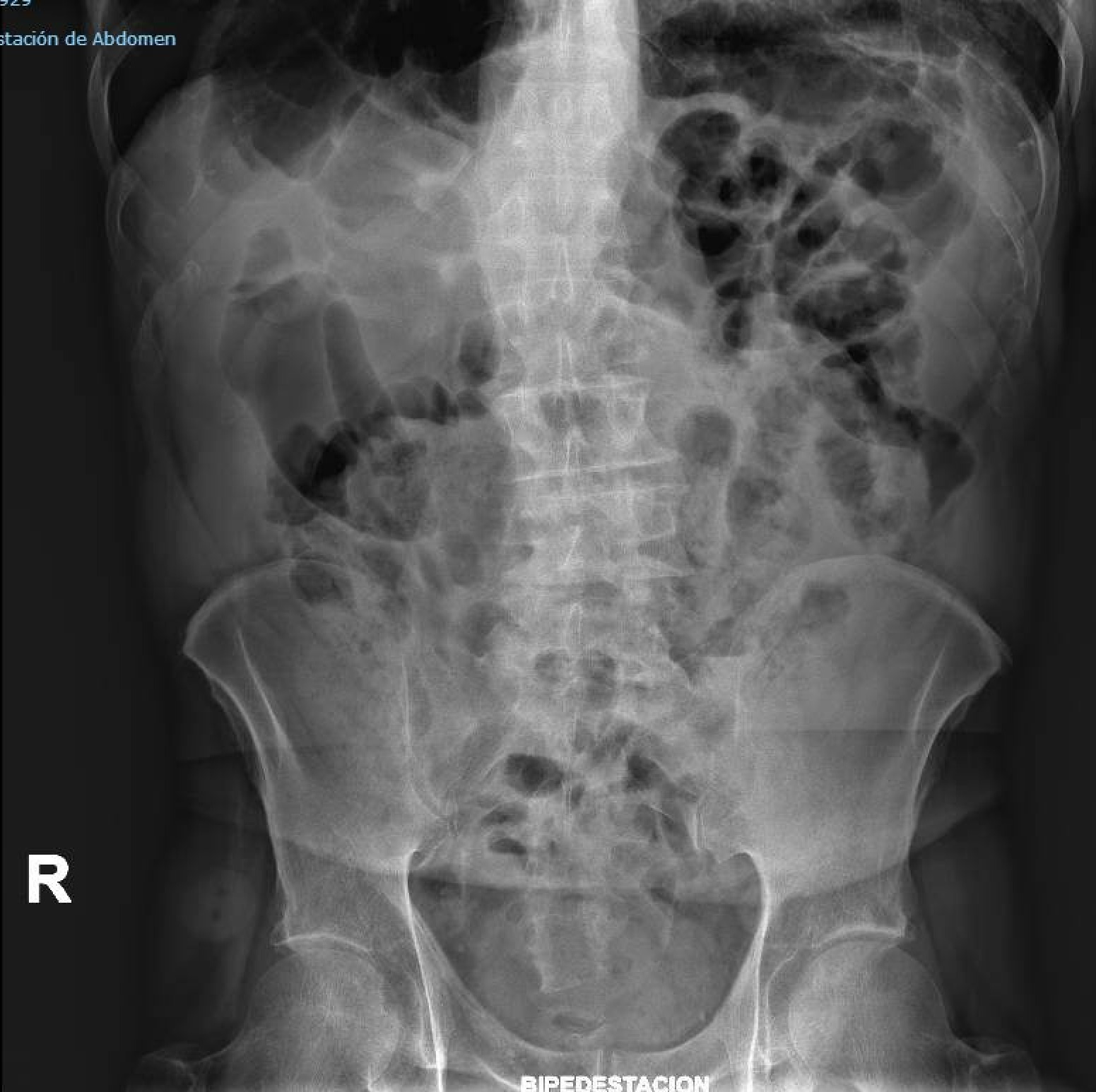
A 75-year-old male with persistent constipation for two weeks, associated with general malaise and generalized abdominal discomfort. A plain abdominal X-ray was performed, which showed abundant fecal content in the colonic loops without ruling out loop suffering, so an abdominal CT scan was requested to complete the study. The CT scan showed a large fecaloma in the upper rectum measuring approximately 10 cm in diameter, as well as abundant fecal matter in the colonic frame, without complete obstruction of the colonic lumen (Figure 1). Despite intensive conservative treatment (oral laxatives, rectal enemas, Gastrografin®, etc.), the patient did not have a bowel movement. After consulting with general surgery and with surgery being the only treatment option, endoscopic disimpaction with Coca-Cola® was decided upon.
Figura 1
Coronal CT scan of the abdomen with contrast. A large fecal impaction measuring approximately 10 cm in diameter is visible in the upper rectum, along with abundant fecal debris in the colonic lumen.

A colonoscopy was performed, revealing a large fecal impaction occupying almost the entire circumference of the colonic lumen, located about 10 cm from the external anal margin. Using a sclerotherapy needle, we proceeded to inject Coca-Cola® into several areas of the fecal impaction, softening the mass, and then, with the help of a wire loop, we achieved almost complete fragmentation of the impaction. Approximately 550 ml of Coca-Cola® was used in the procedure (Figures 2-4).
Figura 2
Endoscopic image of fecal mass approximately 10 cm from the external anal margin that does not completely obstruct the colonic lumen.

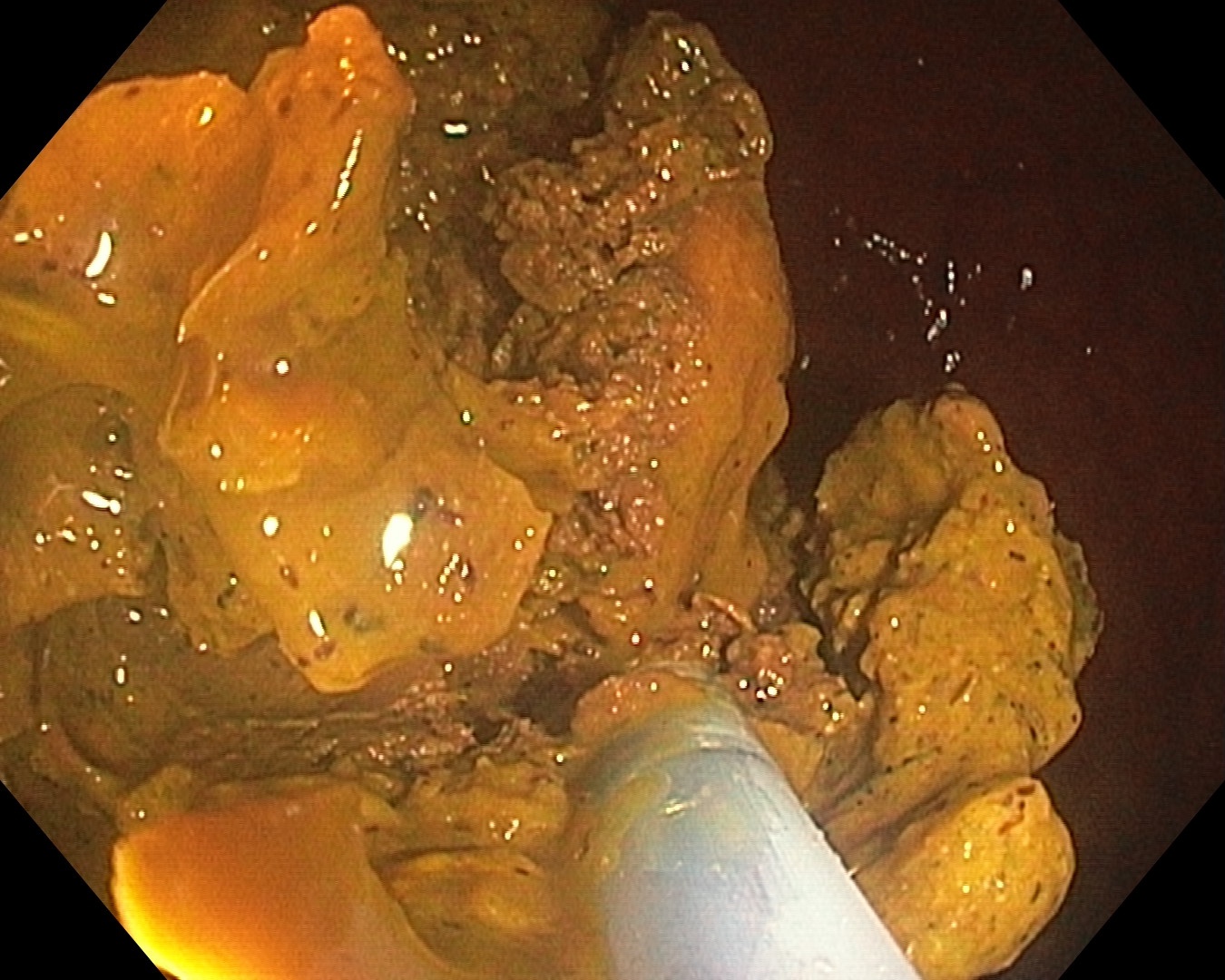
Figura 3
Partial fragmentation of the fecaloma. Small drops of Coca-Cola® are seen in the colonic lumen after injection into the walls of the stool mass.
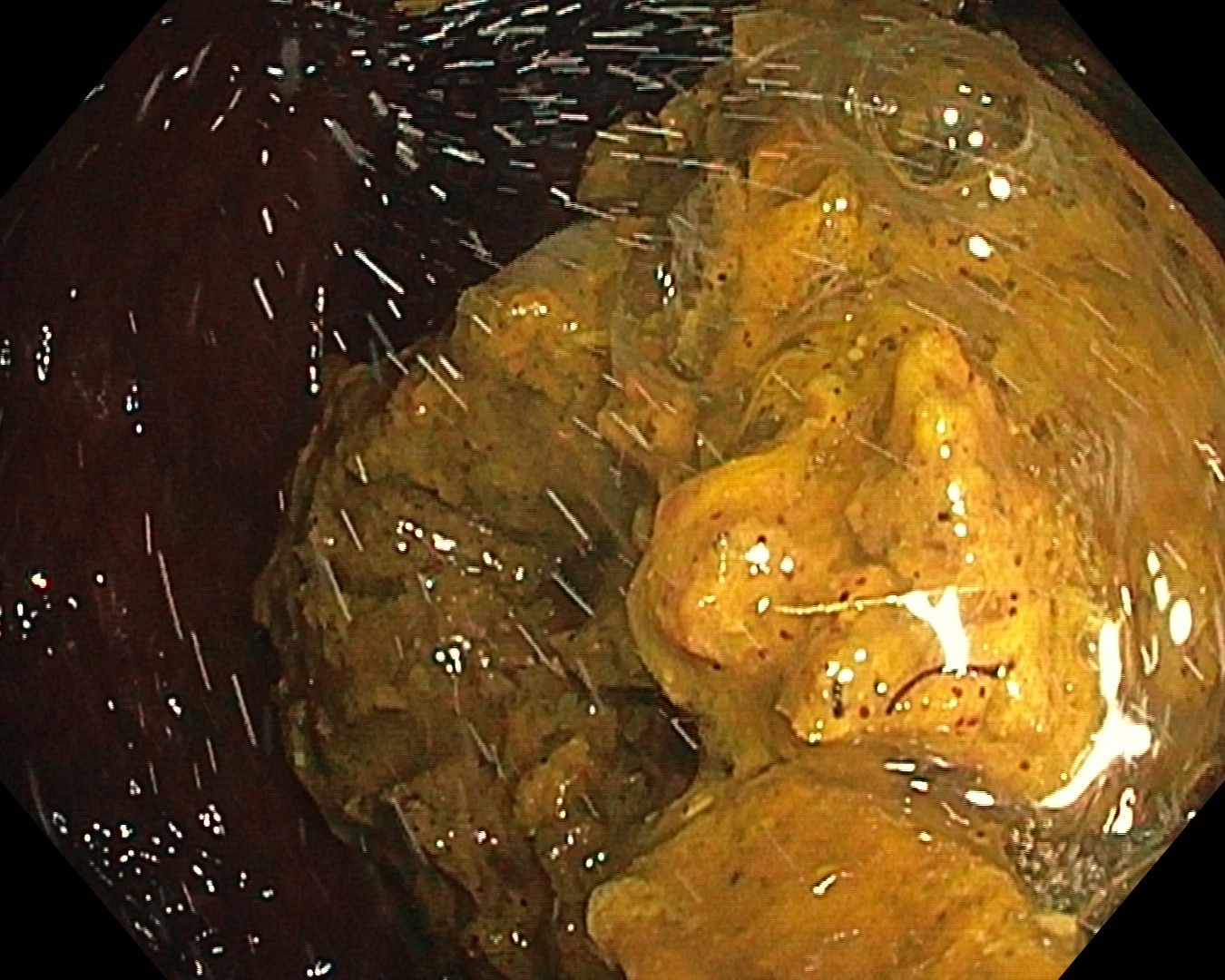
Figura 4
A decrease in the volume of the fecaloma is seen after several injections of Coca-Cola® through its walls.
Following the endoscopic procedure, an enema was administered and oral laxatives were prescribed, with good subsequent progress. A rectoscopy was performed a few days later, which confirmed complete resolution of the fecal impaction and the absence of alterations in the rectal mucosa. The patient was subsequently discharged (Figura 5).
Discussion
Coca-Cola® is a well-known soft drink worldwide. It is used in the field of digestive endoscopy to treat certain gastrointestinal obstructive conditions such as gastric bezoars, thanks to its composition. The acidic nature of the beverage, due to phosphoric acid and carbonic acid, as well as the mucolytic effect of sodium bicarbonate and the carbon dioxide bubbles that penetrate through the microscopic pores on the surface of the bezoar, facilitates its fragmentation[2],[3].
Several studies have documented the use of Coca-Cola® as an effective, safe, and low-cost alternative for dissolving gastric bezoars, constituting the first therapeutic option in many cases. However, evidence on its application in the treatment of fecal impaction is limited, and there are no standardized protocols that support its use in this context.
Fecal impactions are usually resolved with conservative measures such as laxatives or enemas. When these fail, surgery becomes the next therapeutic option[4],[5],[6].
In this clinical case, we present an endoscopic procedure in which the direct injection of Coca-Cola® into the fecal impaction allowed it to soften, facilitating its fragmentation with the wire loop. It is important to note that the beverage did not act alone as a resolving agent, but rather as an adjunct that enabled the success of the endoscopic procedure. We believe that, without this preliminary step, the exclusive use of the loop would not have been sufficient to resolve the problem.
Although the strategy was effective and no lesions were observed in the rectal mucosa in the subsequent follow-up colonoscopy, we believe that it should be used with caution. Extrapolation from cases of gastric bezoars, where there is more evidence, should not be done automatically. This report represents a specific clinical experience and does not allow for general clinical recommendations to be made.
Although it appears to be a safe and effective procedure, a larger number of cases and systematic studies will be necessary to evaluate its safety, reproducibility, and efficacy in the treatment of refractory fecal impactions.