
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITA ESTE TRABAJO
Tinahones Garrido J, Gómez Torres KM, de la Cuesta Fernández I, Viñolo Ubiña C. Dysphagia lusoria: when diagnosis hides in the anatomy. RAPD 2025;48(5):190-192. DOI: 10.37352/2025485.3
Introduction
We present the case of a 53-year-old woman diagnosed with a congenital anomaly that plays an important role in the differential diagnosis of dysphagia, especially in young patients with no preexisting conditions or obvious risk factors for other esophageal pathologies.
Clinical case
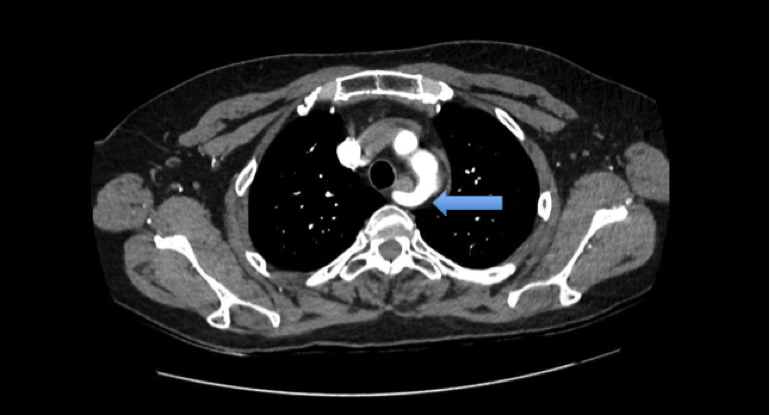
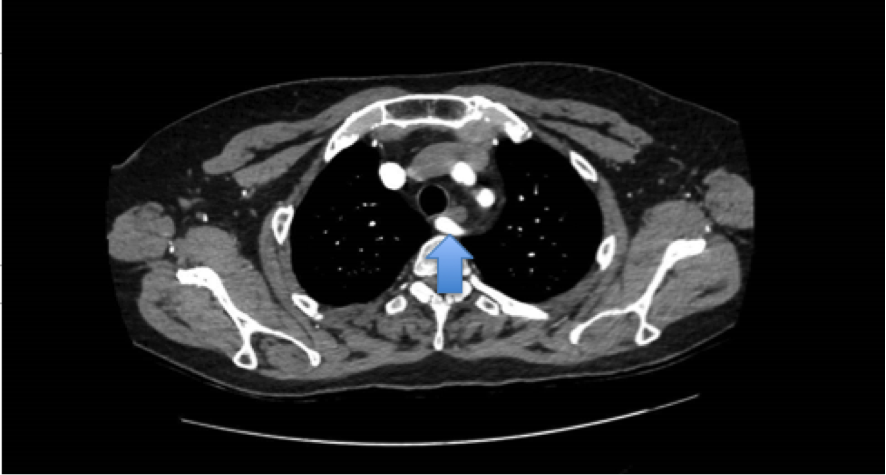
A 53-year-old woman with no relevant medical history was referred from primary care for long-standing dysphagia, initially affecting solids but now also progressing to liquids and accompanied by occasional vomiting and a feeling of a lump in her throat. Given the normal laboratory results and the lack of response to treatment with proton pump inhibitors (PPIs), an upper gastrointestinal endoscopy was requested, revealing a posterior indentation at the level of T3 suggestive of a retroesophageal aberrant right subclavian artery. Following these results, a series of esophagogastroduodenal images was requested, showing the impression caused by extrinsic compression on the posterior wall of the esophagus (Figure 1) and a CT angiogram (Figures 2 and 3), which confirmed the presence of this congenital aberrant artery, originating in the aortic arch, distal to the left subclavian artery and with a retroesophageal course, responsible for the dysphagia she presented. With all this information, the patient was referred to vascular surgery and scheduled for arterial bypass, pending assessment of the technique, with or without endovascular occlusion.
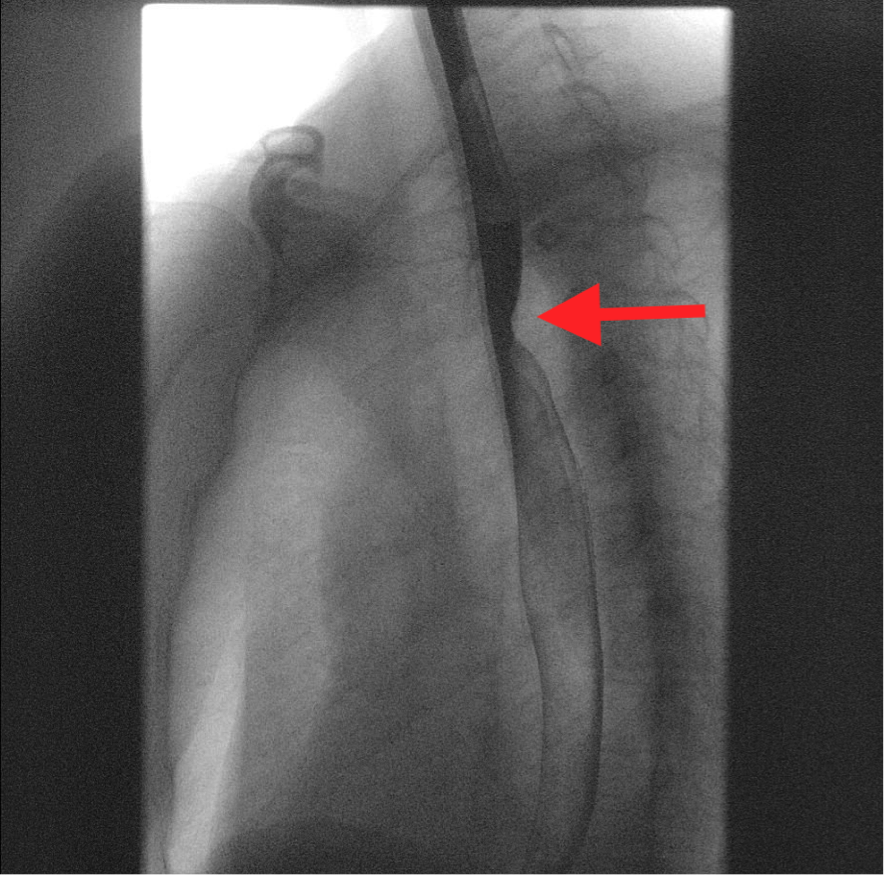
Figure 1
Esophagogastroduodenal series showing extrinsic compression on the posterior wall of the esophagus (red arrow).
Discussion
Esophageal dysphagia can be caused by a variety of factors, including motility disorders, inflammatory diseases, and mechanical diseases. Among the most common causes are gastroesophageal reflux, eosinophilic esophagitis, ingestion of caustic substances, the presence of foreign bodies, achalasia, and extrinsic compressions, including those of vascular origin. It is important to consider vascular causes in the differential diagnosis of dysphagia, especially in young patients without preexisting diseases or obvious risk factors for other esophageal pathologies.
The prevalence of subclavian artery anomaly causing luscious dysphagia varies between 0.5 and 1.8% and is more common on the right side. This condition arises due to the persistence of the seventh right intersegmental artery and abnormal involution of the fourth aortic arch during embryonic development. In 80% of cases, the vessel is retroesophageal, in 15% it is located between the trachea and the esophagus, and in 5% it is pretracheal. The aberrant subclavian artery is often discovered incidentally during imaging tests performed for other reasons, and is usually asymptomatic. However, it can have a significant impact if it causes symptoms by compressing vital structures related to the abnormal path of the vessel (dysphagia if it compresses the esophagus, respiratory distress if it compresses the trachea or pulmonary artery, and even Horner's syndrome if it affects the cervical sympathetic plexus). The average age at which these symptoms begin to manifest is after 50 years of age, which may be related to the loss of flexibility of the esophagus due to aging, increased esophageal compression caused by progressive aneurysmal dilation of the aberrant artery, or stiffness caused by arteriosclerosis in the vessel wall.
Effective management of this condition requires accurate evaluation, including relevant imaging tests such as CT and MRI, which are considered the gold standard. Other tests, such as barium esophagography and endoscopy, remain essential for guiding the initial diagnosis. In addition, a multidisciplinary and personalized therapeutic approach is needed, involving gastroenterologists, radiologists, and vascular surgeons, which will vary depending on the severity, from dietary changes to surgery to ligate or reposition the aberrant subclavian artery and thus relieve the compression.