
 Descargar número completo
Descargar número completo Download full issue
Download full issueCite this work
Vergara Ramos J, Guerrero Palma E, Barba Abad I, Sanabria Marchante I, Macías Rodríguez MA. Small intestine hematoma after bicycle accident. RAPD 2025;48(4):xx-xx. DOI: 10.37352/2025483.4
Introduction
Intramural hematoma of the small intestine is a rare condition in abdominal trauma, occurring in less than 1% of closed trauma cases[1]. It is more common in children than in adults, and most reported cases occur in the duodenum, with jejunal hematoma being very rare[2],[3].
We present a case of a male who, after a trauma while riding a bicycle, presented with overt rectal bleeding due to a jejunal hematoma, diagnosed by video capsule endoscopy.
Clinical case
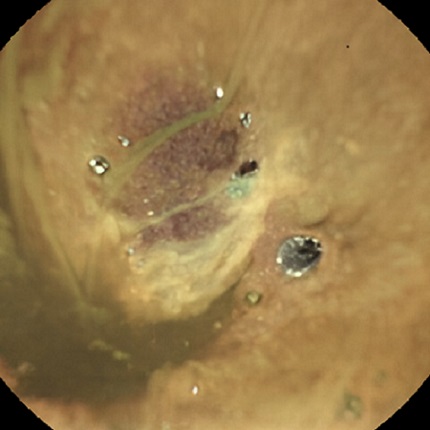
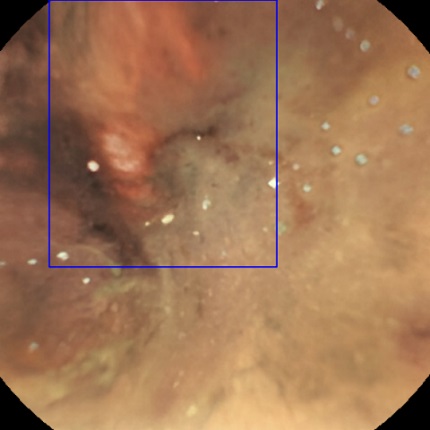
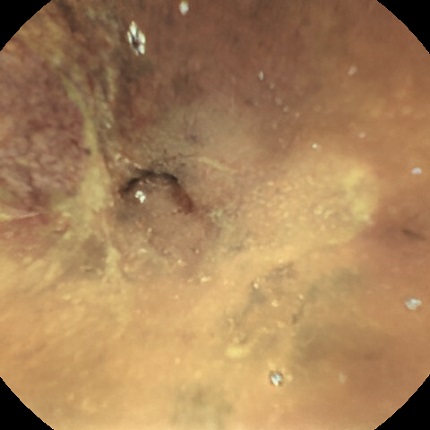
A 50-year-old male with no relevant personal history, who is athletic, presents with overt rectal bleeding, hemodynamic instability, and anemia requiring transfusion. Upon completion of the medical history, he reports that 30 hours ago he accidentally fell from a bicycle from a height of two meters, causing blunt abdominal trauma. After hemodynamic stabilization, an oral endoscopy and colonoscopy were performed, revealing fresh blood in the colon and distal ileum without identifying any active bleeding points or potentially bleeding lesions, only isolated diverticula in the colon that did not show signs of bleeding. Initially, a diverticular origin of the bleeding was considered, but given that the patient continued to have symptoms, and the colonoscopy had revealed abundant blood content in the ileum, it was necessary to rule out a small intestine origin, given the patient's history. It was therefore decided to complete the study with a Navicam SB video capsule endoscope with ProScan artificial intelligence (27 mm long and 11.8 mm in diameter). An extensive area of ecchymotic and markedly congested mucosa was identified in the mid-distal jejunum, with preserved villi and folds and blood remains at that level, suggestive of intestinal hematoma, with no other alterations at other levels, suggesting that this was the cause of the bleeding (Figures 1-3).
Figure 1
Endoscopic video capsule image showing markedly congestive ecchymotic mucosa without active bleeding at the mid-distal jejunum level.
Discussion
The clinical presentation of intestinal hematoma is highly variable and nonspecific, requiring a high degree of diagnostic suspicion. It can range from mild abdominal pain to intestinal obstruction, with rectal bleeding being a very rare and uncommon presentation[3]. The literature suggests that intramural intestinal hematomas are more common in people on anticoagulant therapy, with coagulation disorders, or who have undergone endoscopic procedures. Therefore, a thorough medical history, diagnostic suspicion, and appropriate complementary studies are very important[4].
Although there is no standardized protocol, a conservative approach is usually taken initially, as the outcome is usually favorable, with surgery being reserved for uncontrolled cases.
In this case, we highlight the importance of video capsule endoscopy as a diagnostic tool that allowed us to detect the lesion described, which was causing the clinical symptoms, thus avoiding unnecessary additional tests or new endoscopic studies.