
 Descargar número completo
Descargar número completo Download full issue
Download full issueCORRESPONDENCE
Miguel Ángel Lorente Martínez
University Clinical Hospital San Cecilio. Granada.
18016 Granada
CITE THIS WORK
Lorente Martínez MA, Baute Trujillo EA, Moreno Barrueco M, Martín Navas MA, Candel Erenas JM. Gastrointestinal manifestations of blue rubber bleb nevus syndrome: a case report and literature review. RAPD 2025;48(6):219-221. DOI: 10.37352/2025486.4
Introduction
Blue Rubber Bleb Nevus Syndrome (BRBNS) is a rare condition characterized by the development of multiple vascular nodules on the skin and in the gastrointestinal tract. Although congenital forms exist, most cases are secondary to somatic mutations of genes involved in the regulation of angiogenesis, mainly the TEK gene that encodes the angiopoietin-1 receptor. Its mutation causes permanent activation of the receptor, independent of its ligand, and triggers the uncontrolled proliferation of endothelial cells, responsible for the development of multiple venous malformations[1].
Many patients are diagnosed during childhood, however, they can debut in adulthood in the form of chronic anemia, iron deficiency, or even acute gastrointestinal bleeding.
Clinical case
We present the case of a 40-year-old male with no relevant family history who was being monitored by dermatology due to multiple blue nevi on his skin and was referred to gastroenterology due to a positive fecal occult blood test. The patient described intermittent melena-like stools and occasional episodes of hematemesis. On examination, the abdominal evaluation showed no pathological findings, and the rectal examination was not consistent with melena.
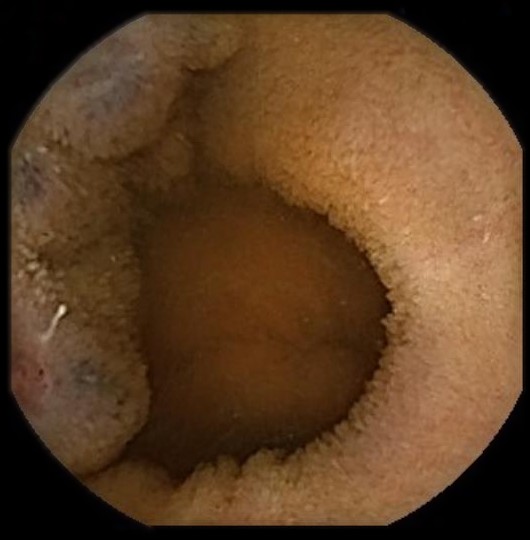
Laboratory tests showed no anemia, iron deficiency, or elevated urea levels. A study was initiated with gastroscopy, colonoscopy (Figura 1), and subsequently capsule endoscopy (Figures 2 and 3) which revealed multiple nevi associated with angiodysplasias throughout the digestive tract.


Given the presence of multiple venous malformations in different areas, the etiological study was completed with genetic analysis (TEK, VHL, etc.), which did not reveal any pathological alterations. The multidisciplinary clinical evaluation ruled out the main diagnostic alternatives (Von Hippel-Lindau syndrome, Osler-Weber-Rendu disease, etc.), establishing the diagnosis of BRBNS.
The patient is currently under close follow-up by the gastroenterology department, maintaining a wait-and-see approach given the absence of clinical and hematimetric repercussions of the gastrointestinal lesions.
Discussion
The diagnosis of BRBNS requires the collaboration of different medical specialties, based on clinical evaluation, endoscopic findings, and genetic studies, although the latter are not essential for diagnosis.
Endoscopic techniques are essential for diagnosing and assessing the extent of the disease and applying therapeutic measures to vascular lesions.
The current lack of scientific evidence makes therapeutic abstention a valid option in mild cases or cases without active bleeding. In cases of bleeding, current studies suggest prioritizing endoscopic therapy (argon plasma coagulation, polypectomy loop excision)[2] over systemic treatments (sirolimus), which are reserved as a second line due to controversy over their safety and management[3],[4].