
 Descargar número completo
Descargar número completo Download full issue
Download full issueCITE THIS WORK
Fernandez Carrasco M, Plaza Fernández A, Sánchez Tripiana M, Diéguez Castillo C. Recurrent digestive hemorrhage due to fundic varices secundary to left-sided portal hypertension after distal pancreatectomy: splenectomy as definitive treatment. RAPD 2025;48(6):222-224. DOI: 10.37352/2025486.5
Clinical Case
A 50-year-old woman with a history of distal pancreatectomy for unilocular acinar cell cystadenoma. She consulted for sudden onset of hematemesis, associated with dizziness and arterial hypotension. Initial laboratory tests showed anemia (Hb 7.1 g/dL) and normal coagulation parameters. Fluid replacement and red blood cell transfusion were initiated.
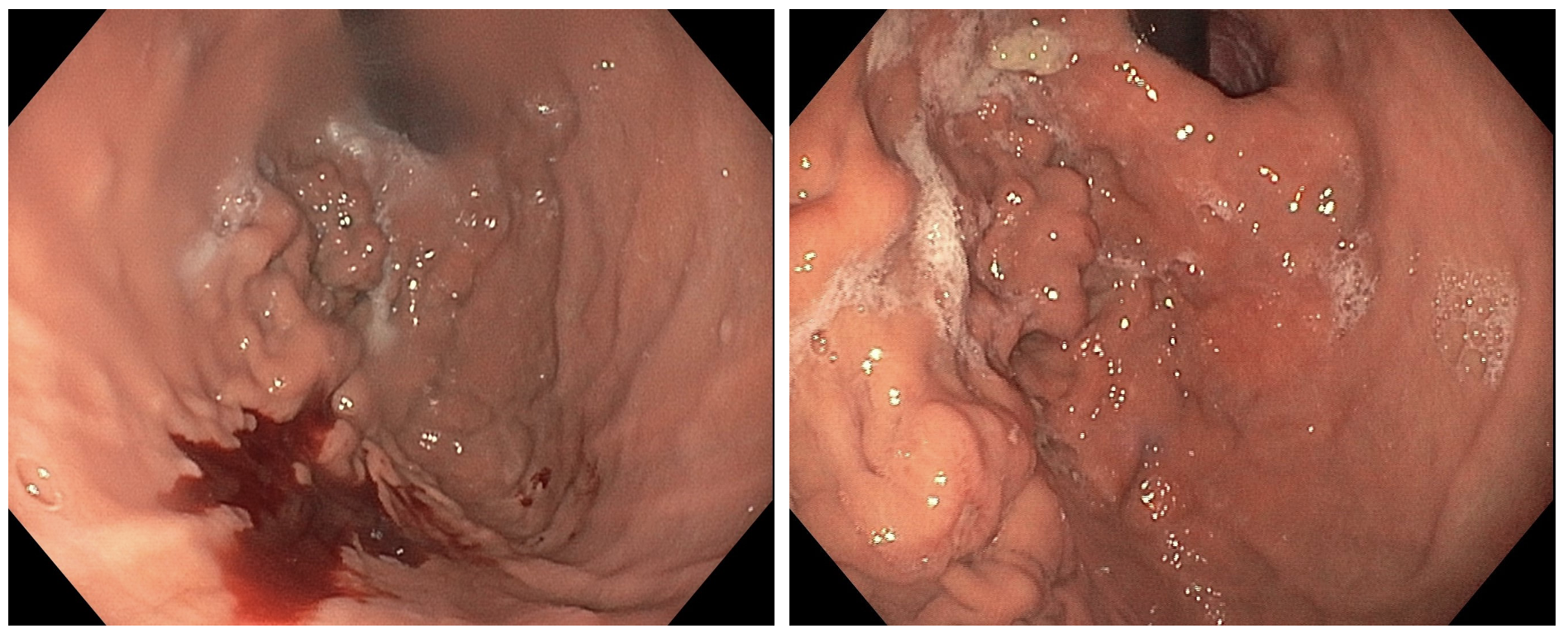
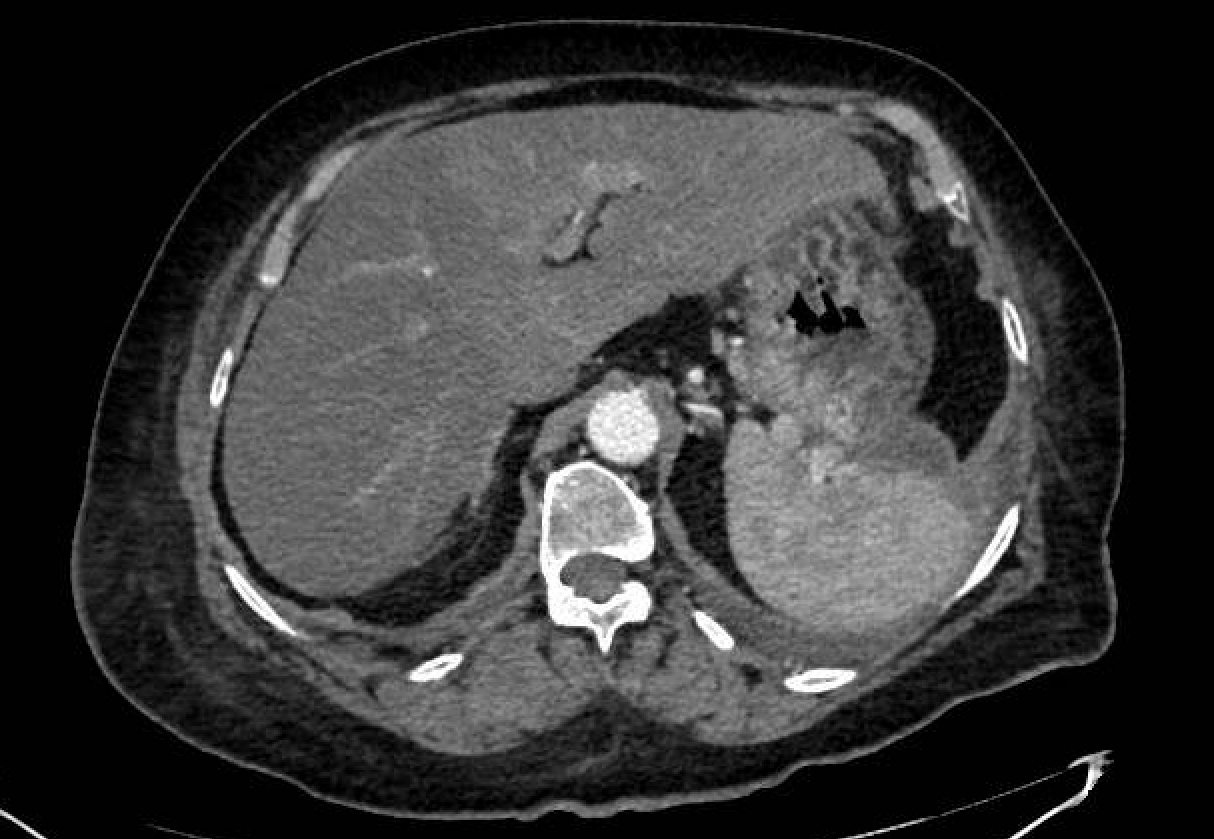
Upper gastrointestinal endoscopy (UGE) revealed the presence of variceal conglomerate in the gastric fundus as the source of the symptoms, and endoscopic administration of cyanoacrylate was performed. Computed tomography (CT) was performed, showing post-surgical changes due to corporocoidal pancreatectomy, numerous splenic venous collaterals, and varices in the fundus and lesser curvature of the stomach. The patient was readmitted one month later due to recurrent bleeding with a new episode of hematemesis and anemia. UGE showed persistent fundic varices. The surgical committee decided to perform a splenectomy as definitive treatment. The patient underwent laparoscopic splenectomy without intraoperative complications. Her progress was favorable, with no new episodes of bleeding during the one-year follow-up period and no increased rate of infections.
Discussion
Segmental extrahepatic portal hypertension can be caused by thrombosis or obstruction of the splenic vein (SV), often due to complications of chronic pancreatitis. Other causes include pancreatic carcinoma, pseudocysts, fibrosis, retroperitoneal tumors, and surgeries such as distal pancreatectomy with spleen preservation, which interrupts splenic venous drainage. Venous obstruction diverts the return from the spleen to vessels with lower pressure, generating collateral circulation and perigastric varices. Ligation of the SV without venous reconstruction increases the risk of increased pressure in this area, with the consequent formation of varices[1].
Symptoms generally do not occur and it is detected incidentally. In some cases (4-17%), it can cause gastrointestinal bleeding due to rupture of gastric varices. Diagnosis is based on endoscopy, ultrasound, and CT, which identifies splenic obstruction, splenomegaly, and collateral circulation[2].
Initial treatment aims to stabilize the patient. Alcohol sclerotherapy, band ligation, and cyanoacrylate are endoscopic options for controlling bleeding. In classic PH, endovascular techniques include transjugular intrahepatic portosystemic shunting (TIPS), which reduces portal pressure, and balloon retrograde transvenous obliteration (BRTO), which is more effective in cardiofundal varices[3].
The non-indication of TIPS in this context is based on the fact that the procedure is not effective in segmental portal hypertension, since the overall portal pressure gradient is not elevated and the cause of gastric varices is localized obstruction of the splenic vein. TIPS diverts the main portal flow to the systemic circulation, but does not resolve the splenic venous congestion or localized hypertension that causes gastric varices in this scenario[1][5]. Therefore, splenectomy is considered the definitive treatment, as it eliminates the source of venous congestion and prevents hemorrhagic recurrence in patients with segmental portal hypertension secondary to thrombosis or compression of the splenic vein. In patients at high surgical risk, embolization of the splenic artery may be considered. This latter option is less invasive but carries a risk of complications such as splenic infarction or abscesses[3].